Possibilities of endobiliary stenting with complex choledocholithiasis
CONFERENCE PAPER
Possibilities of endobiliary stenting with complex choledocholithiasis
Article Summary
- DOI: 10.24969/hvt.2019.160
- Page(s): 217-225
- Published: 15/10/2019
- Views: 5946
- Downloads: 5696
- Keywords: endoscopic papillosphinctertomy, endoscopic lithoextraction, obstructive jaundice, purulent cholangitis, postpapillotomy bleeding.
Address for Correspondence: Orozali Uzakov, International School of Medicine, Bishkek, Kyrgyzstan,
Email: oroz7@mail.ru, Mobile: +996 555484950
FSBI "1409 VMKG MO", Kaliningrad, Russian Federation
International School of Medicine, Bishkek, Kyrgyz Republic
Abstract
Objective: The aim of the study was to increase the effectiveness and safety of endosurgical treatment of choledocholithiasis.
Methods: The set goal is achieved by studying the causes of unsatisfactory results of lithoextractions, improving its tactics and technology. Patients with known predictors of the futility of lithoextraction were excluded from the study. Based on the study of other causes of inefficiency namely strangulation of calculi with a basket, progression of obstructive jaundice, the addition of purulent cholangitis or postpapillotomy bleeding some new tactical rules and endosurgical techniques were formulated. Their effectiveness was tested in group of patients.
Results: When comparing the research and control groups, a decrease in the frequency of endosurgical treatment of choledocholithiasis was revealed.
Conclusion: The effectiveness of the proposed tactical principles and technological techniques has been proved.
Key words: endoscopic papillosphinctertomy, endoscopic lithoextraction, obstructive jaundice, purulent cholangitis, postpapillotomy bleeding
Introduction
Currently, endosurgical treatment of bile duct calculi has become of significance in the treatment of this pathology (1, 2). The introduction into clinical practice of baskets of various sizes and configurations (3-5), various lithotripsy methods (6, 7) considerably increased the possibilities and the safety of their endoscopic debridement. Sufficient clinical material made it possible to significantly improve the “tactics of X-ray endoscopic treatment of choledocholithiasis” (8, 9), assessing its potential (10, 11).
Despite this, there are still clinical observations when it is necessary to perform an open laparotomy with choledocholithotomy sometimes against the background of not only high obstructive jaundice, but also purulent cholangitis, which does not always end in the patient's recovery (12, 13). In addition, while patients with a preserved gallbladder with a risk of open intervention can still be reconciled, then in patients with postcholecystectomy syndrome the need for laparotomy in the conditions of altered anatomical ratios against the background of adhesions in the subhepatic space can hardly inspire optimism.
Of course, the reasons for such unsatisfactory results can be both the lack of competence of both the attending physician and the endoscopist, as well as the lack of tactical principles and technological methods of the discussed treatment method that are scientifically substantiated by appropriate studies. Until now, generally accepted complex clinical observations (14, 15) are recognized as those occurring with high jaundice, complicated, in particular, by disorders in the hemostatic system or purulent cholangitis, relatively large calculi of hepaticocele, not amenable to passage through the distal section of the choledoch and even through the entire common bile duct (CBD). However, as practice has shown, this does not exhaust the list of criteria for “complexity” (16).
In some surgical treatment facilities, the department heads, the clinical management staff adhere to the following algorithm: “the only attempt in endosurgical treatment, in case of failure or when coming across non-standard ratios is laparotomy, choledocholithotomy”. According to the author, this tactic is somewhat simplified in modern conditions, since it does not take into account the possibilities of multi-stage endosurgical treatment of choledocholithiasis with inter-stage stenting, and in patients with high operational risk it needs correction and specification. Undoubtedly, the role of lithotripsy in the effectiveness of the treatment of choledocholithiasis is difficult to overestimate, however, even fragmented calculi must be extracted, before that, it is necessary to reliably capture them and pass through the lumen of the main bile ducts, and therefore the improvement of lithoextraction is relevant.
Methods
Under the supervision there were 562 patients who in the period 2001-2014 underwent hospital treatment at MBUZ "City Clinical Hospital №6 named after N.S. Karpovich ”, city of Krasnoyarsk (2001-2009), Research Institute of the Ministry of Railways under the Russian Academy of Medical Sciences (2001-2013), KGBUZ“ Krasnoyarsk Regional Clinical Oncology Center named after A.I. Kryzhanovsky (2001-2013), KGBUZ Krasnoyarsk Interdistrict Clinical Hospital No. 7 (2001-2013), Siberian Clinical Center FMBA of the Russian Federation (2001-2007), MBUZ GKB No. 1, Krasnoyarsk ( 2000-2005), GBUZ RH "Abakan City Clinical Hospital" (2008-2013), GBUZ RH "Clinical Oncology Dispensary" (2009-2013), MLPU "Sayanogorsk City Hospital No. 2" (2009) , GBUZ "Regional Clinical Hospital of the Kaliningrad Region" (2012-2014) and GBUZ Kaliningrad Region "The Central City Clinical Hospital" (2013), GBUZ Kaliningrad Region "Sovetskaya Central City Hospital "(2013), of the Osh City Hospital (Republic of Kyrgyzstan, Osh, 2012-2014.), Senior Naval Clinical Hospital of the Baltic Fleet (2014.), GBUZ Kaliningrad" City hospital №1 ".
The criterion for inclusion in the study was choledocholithiasis. Since the complex cases of lithoextraction are generally recognized, the authors did not study these patients nor did they study the patients with incomplete (generally or sufficiently) operative access (endoscopic papillosphincterectomy, EPST) to the supraterminal sections of the common bile duct. Thus, the exclusion criteria from the study were:
1) the impossibility of performing EPST;
2) inadequate implementation of EPST *;
3) complete obturation with hepatic choledochus calculus with the impossibility of retrograde contrasting of suprastenotic expansion;
4) obstructive jaundice above 300 μmol / l;
5) uncorrectable disorders in the hemostatic system;
6) purulent cholangitis (before the start of lithoextraction);
7) the development in the process of multi-stage lithoextraction of acute cholecystitis, requiring surgical treatment;
8) the impossibility of conducting the calculi through the retroduodenal or intrapancreatic portions of the bile ducts due to the apparent discrepancy between the size of the calculus and the diameter of the ducts.
Of 562 patients, 2 groups were formed. The first group consisted of patients with endoscopic lithoextraction performed according to the generally accepted methodology (404 observations - 71.9%) (the causes of unsatisfactory results were studied in this group), the second group (158 patients - 28.1%) - using advanced technology and tactics. These groups were compared by the incidence of acute cholangitis and the level of inefficiency of endoscopic debridement of the bile ducts. The first group was divided into 2 subgroups. The first subgroup consisted of 346 patients (85.6% of all patients of the first group) with successful uncomplicated lithoextraction, regardless of its single or multi-phases.
The second subgroup consisted of 58 patients (14.4% of all patients of the first group) in with unsuccessful (23 patients, of whom there was a strangulation in one observation, and 2 after unsuccessful lithoextraction were limited due to age and concomitant pathology to stenting of hepatic choledochus only for stopping obstructive jaundice; the laparotomy and choledocholithotomy were performed in the remaining 20 cases; moreover, 10 patients had anicteric choledocholithiasis, 7 patients had progressive jaundice and 3 cases had non-stopping form) or complicated lithoextraction (as far as purulent cholangitis there were 30 observations, of which 2 patients succeeded in going through lithoextraction against the background of this complication, the postpapillotomy bleeding was revealed in 2 observations and the perforation of the CBD with the development of phlegmon of hepatoduodenal ligament was in 3 observations). In these subgroups, the occurrence of the following morphological features was compared:
1) multiple calculi;
2) calculi that are poorly visualized against the background of CBD;
3) aerobilia;
4) atypical pathological (Mirizzi syndrome) anatomical ratios of the common bile and cystic ducts;
5) atypical forms of calculi;
6) deformations and stenosis of hepatic choledochus;
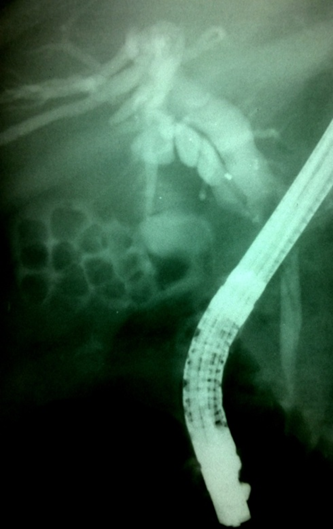
7) high strangulations (Fig.1) due to a peculiar “sludge” of calculi (and not due to the narrowness of the underlying sections of the CBD i.e. endoscopic lithoextraction was not performed in these patients).

We used standard Demling-type papillotomas and Olympus end-face models KD10Q-1, KD411Q, KD29Q. To create a diathermy effect, diathermocoagulators Olympus UES-10 were used. We used nitinol and steel baskets for lithoextraction Olympus, Endo-flex and KARLSTORZ.
Prior to the stent, all patients underwent ECST by cannulation (274 observations - 48.7%) and mixed procedures (pre-dissection, then selective cannulation of the CBD by an arc-shaped papillotome, followed by dissection before visualization of the choledochal lumen) (288 observations - 51.3%). Lithoextraction was carried out in the traditional way - under the control of X-ray, a basket was carried out for a calculus, it was opened, then it was removed with the capture of a calculus or it was opened directly when moving it to a calculus with its subsequent capture.
If it was impossible to remove (infringe) the captured calculus in the duodenum, the following technique was used: the maximally opened basket was moved in the proximal direction, the calculus in this case was partially released from the capture, after which the basket was closed with light traction.
Statistical analysis
Statistical processing of the material was carried out using the statistical software package Statistica 6.0. To compare the frequencies of qualitative characteristics in groups, nonparametric significance criteria were used (Fisher's F-test).
Results and discussion
A study (according to the second subgroup) showed that the reasons for the ineffectiveness of endosurgical treatment of choledocholithiasis were:
1) multiple small and medium (up to 0.8 cm.) calculi that do not leave free space for the basket to fully open (12 observations - 20.7% **);
2) calculi that are poorly visualized against the background of CBD, especially when combined with air that has got into the hepatocholedochus (5 observations - 8.6%);
3) calculi of CBD with atypical anatomical ratios of the common bile and cystic ducts (10 observations - 17.2%);
4) “irregular” *** (cylindrical), cubic, dumbbell shapes, etc. forms of calculi that impede their capture (8 observations - 13.8 %);
5) multiple calculi of “irregular” forms - 5 observations (8.6%);
6) a combination of choledocholithiasis with deformations and stenosis of hepatic choledochus (Fig. 2-4) - 6 observations (10.3%);
7) Mirizzi syndrome, which makes it difficult to determine the anatomical relationships and visualization (Fig. 5) - 7 observations (9.1%);
8) Mirizzi syndrome in combination with calculi of “irregular” form - 4 observations (6.9%);
9) high strangulations of the stone conglomerate (Fig. 1; 6) - 1 observation (1.8%).
A study with Mirizzi's syndrome, which complicates the determination of anatomical relationships and visualization, showed that lithoextraction is absolutely hopeless and very unsafe (of the seven failures, five were complicated by purulent cholangitis, and in one case, intrahepatic abscesses developed against its background). Based on the foregoing, this feature was considered by the authors as a contraindication to retrograde endosurgical treatment.
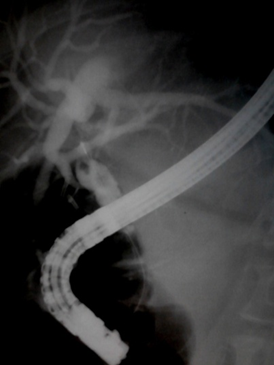

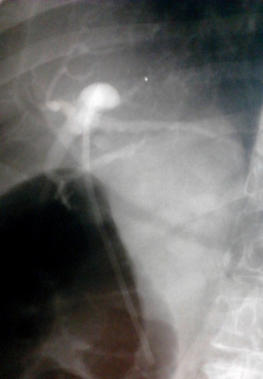

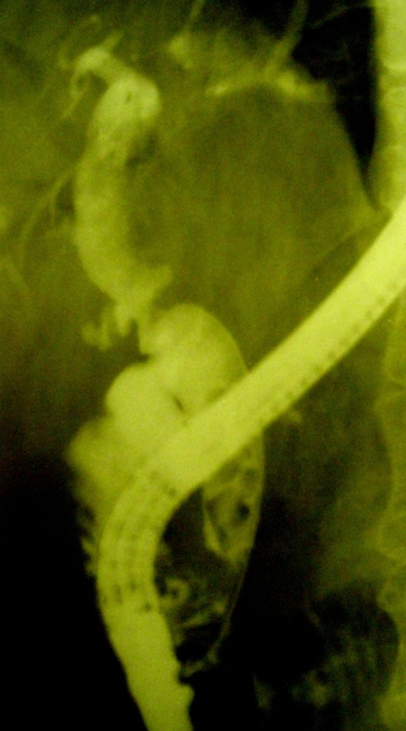
Figure 3. Irregular calculi with hepatic choledochus deformity are determined, limiting the free space for the basket to fully open

Figure 4.The calculus of the common hepatic duct with extended distal stenosis of hepaticocholedoch and its moderate deformity is determined
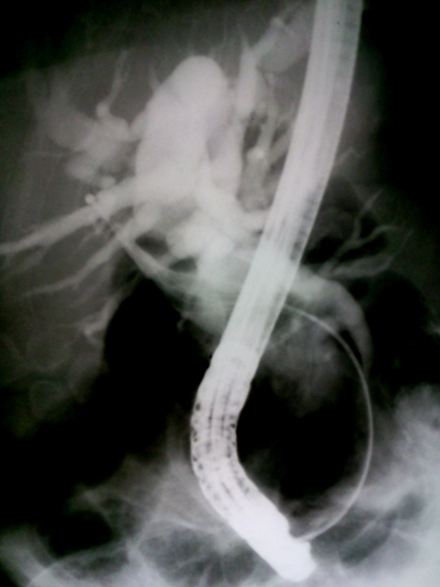
Figure 5. A sharp deletion of hepatic choledochus is determined with the “exit” of the basket beyond its boundaries and non-visualized calculi detected with type 2 Mirizzi syndrome only on laparotomy, choledocholithotomy
In order to overcome the above difficulties, the authors proposed the following set of technological and tactical rules.
In case of multiple calculi, especially of irregular shape, before capturing a distal calculus in order to prevent several stones (Fig. 6) from getting into the basket at once, it is advisable to free up space as much as possible via to the proximal dislocation of a higher lying (Fig. 7) calculus with a half-open basket.




Figure 7. Due to the possibility of capturing two large calculi, the proximal calculus is located upwards, with the distal calculus extracted afterwards, and in the second stage, the proximal one as well.
The analysis showed that simultaneous attempts to completely resolve the bile duct with multiple calculi are accompanied by a decrease in safety due to iatrogenism (perforation of the common bile duct with the development of phlegmon of the hepatoduodenal ligament - 3 observations in the second subgroup (5.1%). In addition, its multi-stage implementation (Fig. 8) is characterized by higher efficiency and safety; however, the inter-stage intervals are complicated by the progression of obstructive jaundice and the addition of purulent cholangitis due to the dislocation of calculi into narrow distal CBD.
Prevention of this complication is achieved due to interstage **** stenting of the main bile ducts, and unlike interstep stenting (as a way to prevent postpapillotomy bleeding) with multi-stage EPST, there is no need for an endoprosthesis of the calculi proximally freely migrating along the choledochus, since the main purpose of this stenting is not only the preservation of the passage of bile, but also the obstruction of migration of calculus into the narrow distal sections of the common bile duct along with its strangulation. Therefore, the stent installed according to these indications should not rise above its retroduodenal part, except for cases of concomitant high stenosis (Fig. 2), and a stone conglomerate strangulated in the supraterminal departments (Fig. 1), when the stent should be conducted above, and it is allowed for it to be conducted into the cystic duct, if the strangulation occurred below its confluence with the hepaticocholedoch.

Figure 8. Multiple calculi of irregular shape are determined, extracted by stages (4 stages).
In case of an unintentional dislocation of the calculus in the common hepatic duct or in the area of high stenosis of the main bile ducts (Fig. 9) or when deliberately pushing in order to free up space to capture the "distal" calculus (Fig. 10) after its extraction, it is advisable to stop lithoextraction. Then offer the patient as much as possible his/her condition allows it, to stay in upright position (it’s better to walk), and resume lithoextraction after 4 hours or the next day, when the calculus migrates on its own to more dilated distal areas.

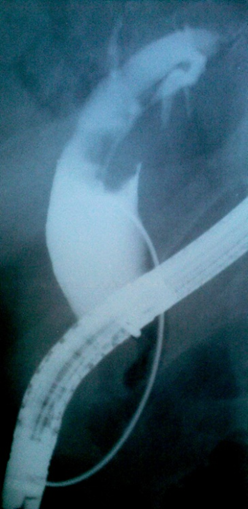

Figure 10. Intentional dislocation of the proximal calculus into the common hepatic duct
When conducting a calculus through the retroduodenal and intrapancreatic departments of the common bile duct, it is advisable to change the direction of traction parallel to the bend of the choledochus.
Evaluating the effectiveness of each element of the proposed algorithm is an insoluble task (to obtain representative groups is hardly feasible even with multicenter research) and the meaning of this is very doubtful, since all elements are interconnected and consistently applicable, therefore they were evaluated in a complex (Table 1). The incidence of the above reasons for the inefficiency of endoscopic lithoextraction (according to the studied group) and their structure in the study and comparison groups is not statistically significant (Table 2).
|
Table 1. Comparison of the efficacy and safety of endoscopic lithoextraction of calculi of the main bile ducts according to traditional and advanced tactics |
||||
|
Groups |
Evaluation parameters |
|||
|
Efficiency |
Level of complications |
|||
|
Absolute number |
% |
Absolute number |
% |
|
|
Study group N=404 |
349 |
86.4 |
35 |
8.7 |
|
Comparison group N=158 |
151 |
95.6 |
5 |
3.2 |
|
Study group without patients with Mirizzi's syndrome, which complicates the determination of anatomical ratios and visualization, N = 397 |
342 |
86.1 |
30 |
7.6 |
|
Comparison group without patients with Mirizzi's syndrome, which complicates the determination of anatomical ratios and visualization, N = 155 |
148 |
95.5 |
5 |
3.2 |
|
Note. The significance of differences between the study and comparison groups, both with the inclusion of observations with Mirizzi's syndrome (p =0.0007 in efficiency, p =0.0007 in safety) and without inclusion (p = 0.014 in efficiency, p = 0.04) is statistically significant.
|
||||
As it is obvious, according to Table 1, the efficiency increased by 9.8% with an increase in safety by 5.5%, and on the condition of exclusion from both groups of patients with Mirizzi's syndrome, which complicates the determination the anatomical ratios and visualization (the authors consider this feature as a contraindication to endoscopic lithoextraction) by 9.4% and 4.4%, respectively. When comparing patients with identified reasons for the decrease in the efficiency of endoscopic lithoextraction of the first (the second subgroup with the exception of patients with Mirizzi's syndrome, which complicates the determination of the anatomical ratios and visualization - 51 patients) and the second group (also with the exception of patients with Mirizzi's syndrome, which makes it difficult to determine anatomical ratios and visualization - overall 19 patients) an even more pronounced advantage was revealed of the proposed tactics (Table 3): increased efficiency by 72.1%, safety - by 32.5%.
|
Table 2. The occurrence and structure of the reasons for the decrease in the efficiency of endoscopic lithoextraction in the study and comparison groups |
||||
|
The reasons for the decrease in the effectiveness of endoscopic lithoextraction. |
Occurrence |
|||
|
Study group, n=404 |
Comparison group, n=158 |
|||
|
Absolute N |
% |
Absolute N |
% |
|
|
Multiple small and medium (up to 0.8 cm) calculi that do not leave free space for the basket to fully open |
12 |
3.0 |
5 |
3.2 |
|
Stones that are poorly visualized against the background of CBD, especially with a combination of air trapped in the hepaticocholedochus |
5 |
1.2 |
2 |
1.3 |
|
CBD calculi with atypical anatomical ratios of the common bile and cystic ducts |
10 |
2.4 |
3 |
1.9 |
|
“Irregular” forms of calculi that make them difficult to capture |
8 |
2.0 |
4 |
2.5 |
|
Multiple calculi of "irregular" forms |
5 |
1.2 |
3 |
1.9 |
|
The combination of choledocholithiasis with deformations and stenosis of hepatic choledochus |
6 |
1.5 |
2 |
1.3 |
|
Mirizzi's syndrome, which complicates the determination of anatomical ratios and visualization |
7 |
1.7 |
3 |
1.9 |
|
Mirizzi's syndrome in combination with calculi of the "irregular" form |
4
|
0.9
|
2
|
1.3
|
|
High strangulation of calculae conglomerate |
1 |
0.2 |
1 |
0.7 |
|
Table 3. Comparison of the efficacy and safety of endoscopic lithoextraction of calculi in patients with various reasons for reducing its effectiveness |
||||
|
Patients with various causes of decrease in efficiency and safety of lithoextraction |
Evaluation parameters |
|||
|
Efficiency |
Level of complications |
|||
|
Absolute N |
% |
Absolute N |
% |
|
|
Patients from the second subgroup, N = 51 ***** |
3 |
5.8 |
30 |
58.8 |
|
Patients from the comparison group, N = 19 ****** |
12 |
78.9 |
5 |
26.3 |
|
Note. The significance of differences in efficiency of p=0.0001, and in safety of p=0.015 is statistically significant
|
||||
* The criterion for inadequate performance was the inability to visualize the lumen of the choledochus through the papillotomy fistula or enter at an angle close to the straight one into the choledopapillotomy
** The relative distribution is provided within the second subgroup
*** The correct form of calculus in the framework of this article was considered round and ovoid
**** It should not be confused with interstep stenting as a way of preventing postpapillotomy bleeding during two-stage EPST – endoscopic papillosphincterectomy
***** 7 patients from the comparison group with Mirizzi's syndrome, which complicates the determination of anatomical ratios and visualization, are not included
****** 3 patients from the study group with Mirizzi's syndrome, which complicates the determination of anatomical ratios and visualization, are not included
Conclusion: Mirizzi's syndrome, which complicates the determination of anatomical ratios and visualization, is an absolute contraindication to endosurgical retrograde treatment of choledocholithiasis. The maximum uncoupling of multiple calculi for the isolated capture of each with their multi-stage lithoextraction and inter-stenting, which does not prevent the migration of calculi into the most dilated sections of the main bile ducts in the inter-stage intervals, changing the direction of traction of the captured calculus in parallel to the bend of the choledochus makes it possible to increase the efficiency of the endoscopic retrograde lithoextraction by 9.4% , and security by 4.4%.
Conflict of interest: None to declare
Authorship: V.V. Y., O.J. U. equally contributed to the study and preparation of manuscript
Acknowledgement and funding: None to declare
References
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
