From Editor-in-Chief: On issue, our rank – trail of pandemic period but increase in quality and SDG, congresses, trials, guidelines and important documents, news on prevention
EDITORIALS
From Editor-in-Chief: On issue, our rank – trail of pandemic period but increase in quality and SDG, congresses, trials, guidelines and important documents, news on prevention
Article Summary
- DOI: 10.24969/hvt.2025.572
- CARDIOVASCULAR DISEASES
- Published: 11/06/2025
- Received: 08/06/2025
- Accepted: 09/06/2025
- Views: 3380
- Downloads: 2777
- Keywords: Biomedical publishing, journal`s performance, citation analysis, peer-review, surgery, vascular diseases, cardiology, arrhythmias, interventions, imaging
Address for Correspondence: Gulmira Kudaiberdieva, Editor-in-Chief, Heart, Vessels and Transplantation
E-mail: editor@hvt-journal.com
ORCID: 0000-0002-4794-8435, 0000-0003-4099-8816 Scopus ID: 7003985934
Editorial

From Editor-in-Chief: On issue, our rank – trail of pandemic period but increase in quality and SDG, congresses, trials, guidelines and important documents, news on prevention
Key words: Biomedical publishing, journal`s performance, citation analysis, peer-review, surgery, vascular diseases, cardiology, arrhythmias, interventions, imaging
Dear readers,
With wishes of pleasant summer and vacation season for our readers above equator and productive winter season for all the rest.
I share with you our rank and performance indicators published by databases, content of current June 2025 issue, new guidelines and consensus documents, and new important studies and news on COVID prevention policies.
The performance indicators of journals for the year 2024 have been released by SCOPUS and SCIMAGOJR
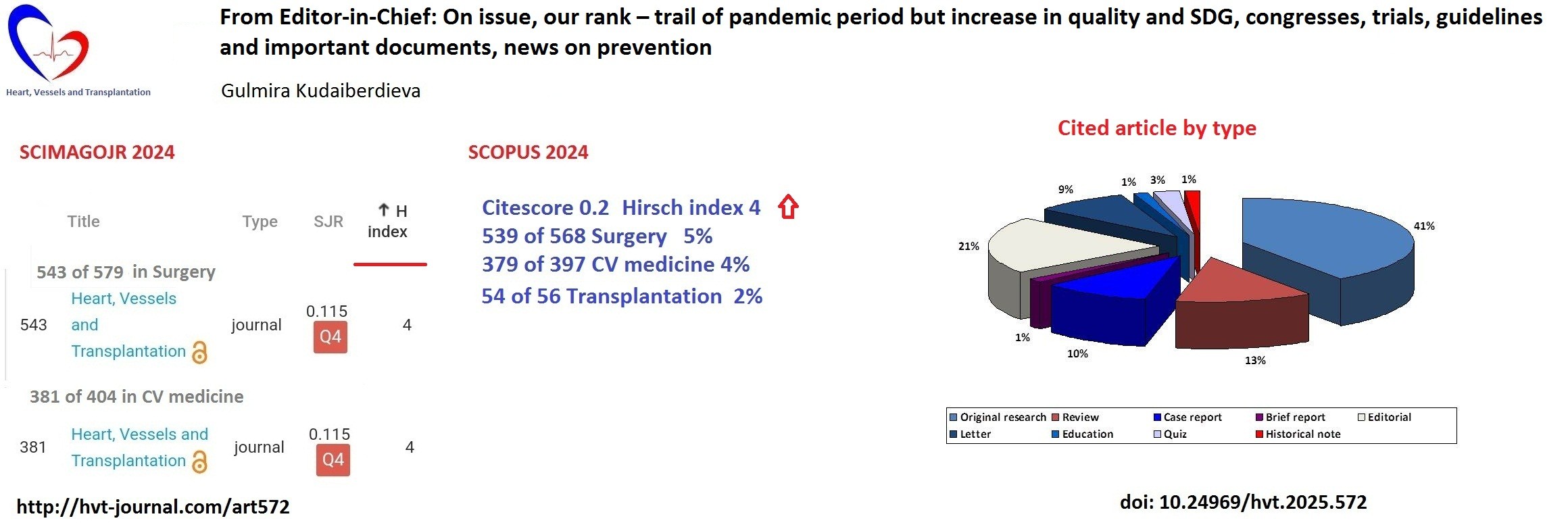
The SJR reduced to from 0.118 to 0.115 for all our categories: surgery, CV medicine and transplantation, we still in Q4, but we sustained the SCOPUS CiteScore 0.2 for all categories , and increased our Hirsch index from 3 to 4 and increased number of articles cited and number of citations (Fig. 1).
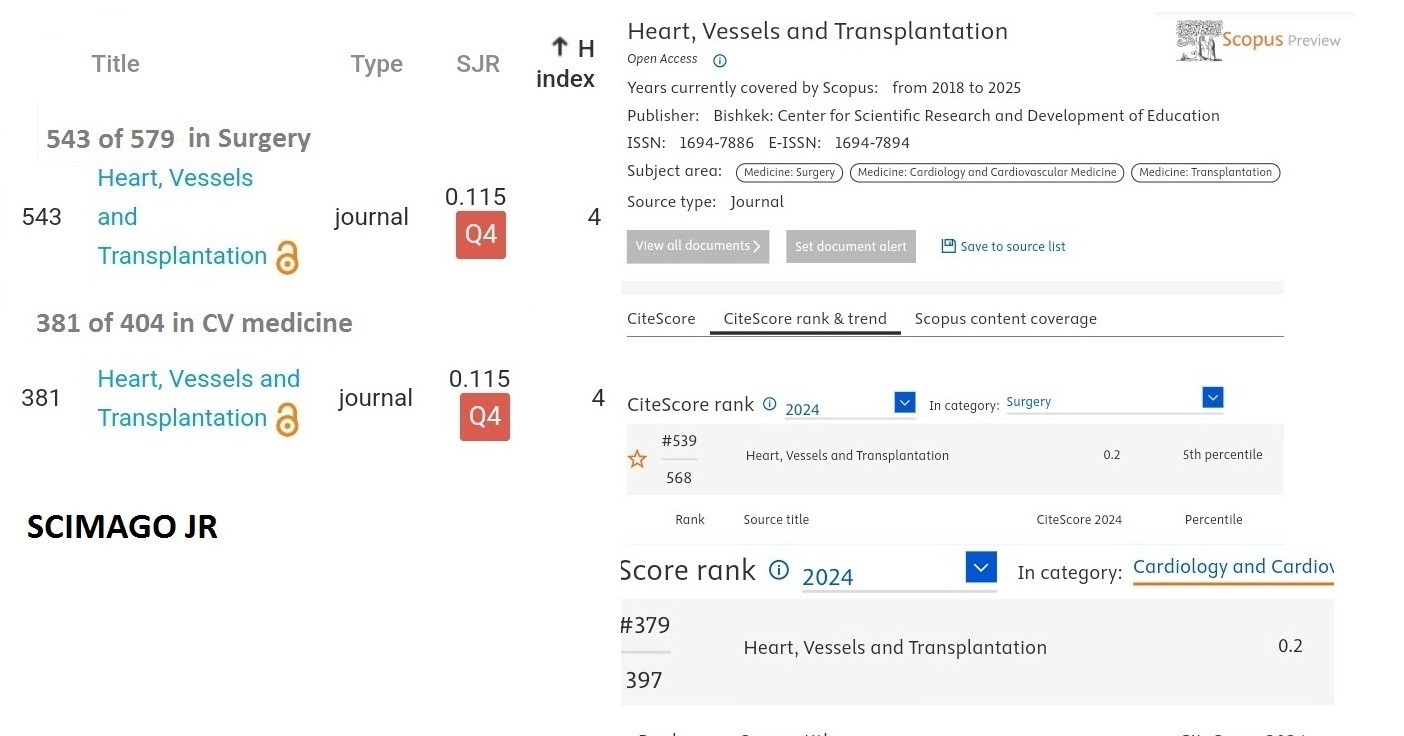
Figure 1. 2024 SCIMAGOJR rank by H-index (left) and 2024 SCOPUS CiteScore rank (right) of Heart, Vessels and Transplantation (modified from references 1 and2)
Ranking by SJR in cardiovascular (CV) medicine was 357 of 388 in 2023 and 381 of 405 in 2024, surgery - 517 of 549, 547 of 580 journals and transplantation – 50 0f 53, 54 of 56, respectively. Though the number of journals has changed for past year, we slide slightly down – the gap between us and the last journal in the list become shorter, we were higher by more than 31-32 now 23-24. The percentiles decreased from 6 to 5% in surgery and 5 to 4% in CV medicine.
But we have increase in cited articles (80 now) citations number (now over 120) and H-index (from 3 in 2023 to 4 in 2024)– meaning the cited articles number and quality of cited articles has increased.
All indices like SJR, CiteScore, SNIP, Hirsch index are based on citations.
To seek some explanations for SJR dynamics we made further analyses. If we look at citation dynamics 2018-2025 provided by SCIMAGOJR (Fig. 2), we can see that citations number per document sharply decreased during pandemics 2020-2023, then our decline in SJR and percentile may be explained reduction of citations between 2021 and 2023 – composite for metrics in 2024. In 2024 and already in 1st quarter of 2025 we observe marked increase in citations per document.
Several observational studies and systematic analyses reported the impact of pandemics on citations (3-5). Citations to the COVID content articles increased and to nonCOVID articles decreased. Whittaker et al. (4) analyzed citations for 17 million papers for 2020-2022 and revealed that among papers with at least one citation published in NEJM and Lancet, 53% were COVID preprint articles while only 12% were nonCOVID articles. Brandt et al. (5) analyzed citation rates of COVID and non-COVID articles published in 24 journals and found that median citation rate of COVID articles was 6 times higher than non-COVID articles – 120.79 vs. 21.63.
Our empirical citations data show similar pattern. In 2020, we had more cited articles and articles with several citations, among cited articles published in 2020, we have five cited articles on COVID and 3 of them received 2 and more citations (4, 3, and 2 citations).
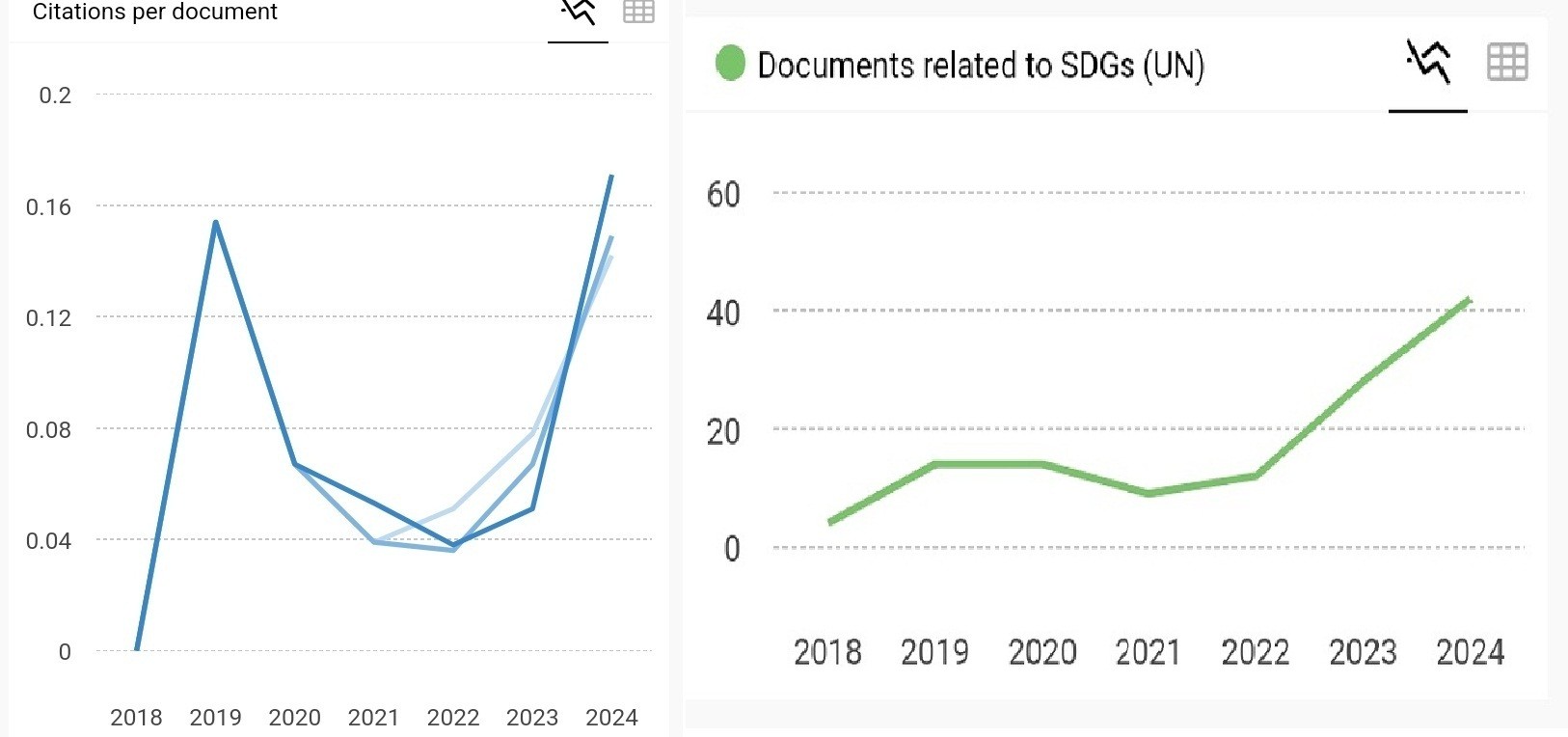
Figure 2. Time trend of Citations per document and Documents related to SDGs (modified from reference 1).
However further in 2021, we see the reduction of overall citations and in 2022, we have articles only cited once. Thus, 2021 and 2022 contributed to lower SJR and percentiles.
We have to acknowledge that we increased number of published articles the denominator for CiteScore, but it is still 02. In balance as we have increase in citations.
If we analyze cited articles (Fig. 3) we see that 23% of our 344 articles indexed in SCOPUS (2018-2025), received citations. The 25% of articles received more than one citation and 75% are cited once, therefore 1/4 of them are articles of better quality. It corroborates with increase in Hirsch index from 3 to 4 in 2024, meaning that we have top 4 articles of good quality that were cited 4 times. If we look at the types of cited articles, we see that 41% of them are original research articles, 14%-reviews, 10% - case reports and 21% Editorials, 9% letters and rest are brief report, quiz articles, education and historical note. These results mean that new scientific evidence as research articles, brief reports or synthesis of knowledge as reviews, and challenging clinical cases, their discussion in form of editorials and letters, editorials, quizzes, historical note on advancement of clinical knowledge and continuous medical educations –are of scientific value, and of interest for medical education and practicing physicians communities. Our articles contributed to the pool of evidence-based knowledge. Increase in UN SDGs articles means that we published more articles on CV disease prevention and health policies aid at improvement of health in frame of UN sustainable development goals.
The citation per document curve goes up; in the 1st quarter of 2025, we have already marked increase in citations and citations per document. We have to continue working hard on selecting the best.
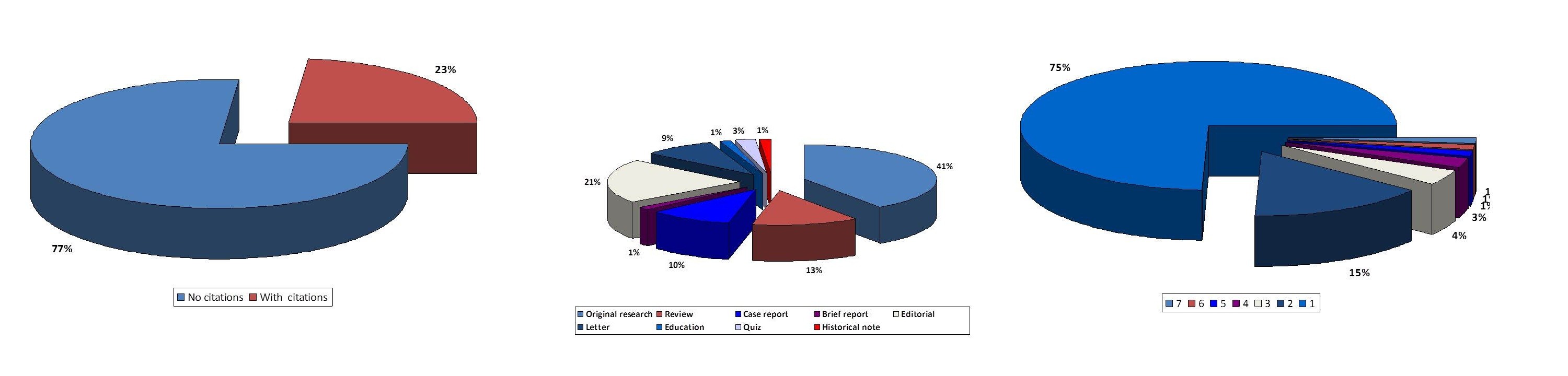
Figure 3. Cited articles by type and number of citations
In current June 2025 issue of our journal, we bring to your attention Editorials presenting new consensus documents that might be useful for all practicing physicians and worth to read on: how to treat cardiogenic shock, on how to visualize and manage infective endocarditis in patients with implanted devices and how to manage left ventricular assisted devices, prepared by our editors and invited experts. We published several original research articles that might be of interest for researchers and physicians: on diagnostic accuracy of GERONTONET ADR tool in prediction of adverse drug reactions and elderly; predictors of Q wave development in ST-elevation myocardial infraction (STEMI) patients who underwent primary percutaneous intervention (PCI) and their association with angiographic findings; effects of phototherapy on hemodynamic parameters in patients with rheumatic arthritis; prevalence of cardiovascular (CV) risk factors in patients with pre-dialysis chronic kidney disease; impact of obstructive sleep apnea on coronary artery disease outcomes; CV disease epidemiology and brief report on attitude of thoracic surgeons on evidence-base practice. You can also find review articles on contemporary interdisciplinary issues: ethical, legal and environmental angles of organ transplantation; ecology, education and health; and diagnostic imaging of hepatic alveolar echinococcosis - parasitic disease that has endemic incidence and finally case report on how to perform ablation in presence of septal occluder in patient atrial fibrillation and letters discussing this complicated and successfully treated case.
Among the recent trials presented this spring at ACC 2025 scientific sessions in Chicago, USA that caught my attention are: SOUL, ZENITH, TRILUMINATE and ADVANCE HTN.
Oral semagludite, a glucagon like peptide 1 receptor agonist (GLP -1) in randomized placebo controlled SOUL trial (6) including 9260 patients with diabetes and CV disease and/or chronic kidney disease, reduce major adverse CV events (CV death, nonfatal myocardial infarction and nonfatal stroke) by 14% (HR – 0.86, 95%CI- 0.77-0.96, p=0.006). It was also safe as adverse events was lower in semaglutide group than in placebo one.
Another ADVANCE HTN study (7), concerns population of patients with uncontrolled hypertension. Lorundrastat a new drug with different from aldosterone receptor antagonists target -the aldosterone synthase inhibitor, reduced significantly blood pressure in patients with uncontrolled hypertension as compared to placebo. It was used as 50 mg per day and increased dose up to 100 mg, if control of blood pressure was not achieved during 12 weeks of treatment, The blood pressure reduction was twice higher that in placebo by 15.4 mmHG (p=0.001), in dose adjustment group it was 13 mmHG (p=0.006) and in placebo - 7.4 mmHg. The potassium levels should be monitored, as there was an increase in its levels above 6 mmol/l in 5 of 95 patients in the 50 mg daily group.
In ZENITH trial (8) sotatrecept an acitivin-signaling inhibitor added to triple of double therapy in patients with pulmonary arterial hypertension and high risk of death, WHO FC II-IV – reduced composite risk of death, lung transplantation or hospitalization by 76% (HR) during 1 year of follow-up (HR – 0.24, 95%CI 0.13-0.43, p<0.001), with 17.4% of events in treatment and 54.&% in placebo group during 11 months follow-up. It was previously shown to be effective in patients with WHO FC I-III.
The TRILUMINATE trial (9) demonstrated efficacy of tricuspid valve edge-to edge repair (T-TEER) in patients with severe tricuspid regurgitation (TR). T-TEER resulted in reduction of TR severity in 87% of patients and improvement quality of life and health status of patients. At 2 years after procedure, freedom from mortality, tricuspid valve surgery and re-intervention was significantly higher in T-TEER than control group ( 77.6% vs 29.3%, p<0.0001).Thus we have more evidence for less invasive treatment for patients with severe TR.
SMART-CHOICE 3 (10) study showed the benefit of monotherapy with clopidogrel over aspirin after DAPT therapy in patients who underwent PCI and are at risk of recurrent events (complex coronary lesions, diabetes and previous myocardial infarction (MI), who completed DAPT). Overall, 5506 patients were randomized for oral intake of 75 mg clopidogrel or 100 mg aspirin daily. During 2.3 years of follow –up the composite of all-cause death, MI or stroke was 4.4% in clopidogrel group and 6.6% in aspirin group (p=0.013). Bleeding rate did not differ between groups. Lower rate of composite event was mainly due to low mortality and MI. These results may not only be projected to patients with complex lesions and high risk of re-thrombosis as MI and diabetes, but also to patients who become intolerant to aspirin or developed resistance to aspirin.
Recent BROADWAY RCT (11) demonstrated cholesterol ester protein inhibitor obicetrapib is effective in reduction of low-density lipoprotein cholesterol (LDL) in patients with atherosclerotic CV disease and familial hyperlipidemia. LDL was reduced by 29% during 81 day of treatment as compared to placebo (2.7%), difference 32.6% (CI 35.8—29.5%), p<0.001.
During ACC 2025, the acute coronary syndromes (ACS) 2025 guidelines (12) was published and our editors and invited experts are in preparation of editorial on new recommendations for ACS treatment in ACC guideline as well as in forthcoming ESC 2025 ACS guideline.
In parallel with EHRA congress 2025, several consensus and position documents were published (13-17) and we recommend to read, study and implement in your practice. The EHRA document on conduction pacing and T-TEER in presence of devices with right ventricular leads will be presented by our Editors in the next September 2025 issue (14, 16).
The document on epicardial ablation of ventricular arrhythmias (VA) (13) covers the all aspects of from indications to ablation procedure of arrhythmias with epicardial substrate The epicardial ablation should be considered for patients with presence of epicardial substrate rather than endocardial or septal intramural; patients with VA predisposed to epicardial involvement- with nonischemic cardiomyopathy, Chagas disease, arrhythmogenic right ventricular dysplasia and Brugada syndrome. The document provides detailed and concise description of indications, anatomy, electrocardiographic, mapping and imaging criteria for identification of epicardial substrate and differentiation from other locations, periprocedural management and ablation techniques.
The EHRA consensus document on antiarrhythmic drugs (AAD) 2025 (15) provides the guidance on classification, mechanisms of action, indications for use, use for arrhythmia acute termination and maintenance of rhythm, prevention and side effects of AAD, in special populations in the era of ablation and device therapies, new AADs. It introduces the new concept of ABC framework:
A-appropriate therapy, when AAD therapy is the best option;
B-as adjunctive therapy to invasive procedures as ablation;
C-complementary with other therapies.
The document on artificial intelligence (AI) use in electrophysiology provides insights on the use of AI for atrial fibrillation detection using photopletismography – present in wearable devices as watches and smartphones; electrocardiogram algorithms for diagnosis of atrial and ventricular arrhythmias,, AI models for prediction of sudden cardiac death and AI tools for guiding of electrophysiological procedures, mapping and ablation, device implantation (17). Recommended AI tools are friendly and help physician to provide best care for patients.
The KDIGO guideline on management of chronic kidney disease 2024 (18) deserves attention as it covers the populations with CV disease, diabetes and use of CV drugs for kidney disease patients. The indications for renin-angiotensin-system (RAS) drugs (angiotensin converting enzyme inhibitor and angiotensin receptor blockers) and sodium glucose co-transporter 2 inhibitors use in patients with chronic kidney disease, CKD associated with CV diseases and diabetes are of interest for our readers, as well overall knowledge on CKD management. There are changes regarding monitoring and withholding treatment with RAS drugs: estimated glomerular filtration rate is the guiding parameter instead of creatinine level.
Finally, there are changes in recommendation for COVID vaccinations, visit the CDC site (19) and check your local agencies, as the populations at high risk are usually also your patients with comorbidities or pediatric population.
Gulmira Kudaiberdieva
Editor-in-Chief
Heart, Vessels and Transplantation
Peer-review: Internal
Conflict of interest: None to declare
Authorship: G.K.
Acknowledgements and funding: None to declare
Statement on A.I.-assisted technologies use: We declare that we did not use AI-assisted technologies in preparation of this manuscript
Data and material availability: Do not apply
References
| 1. SCIMAGOJR. Available at: URL: https://www.scimagojr.com | ||||
| 2. Scopus sources. Available at: URL: https://scopus.com/sources | ||||
| 3.Park S, Lim HJ, Park J, Choe YH. Impact of Covid 19 pandemic on biomedical publications and their citations frequency. J Korean Med Sci 2022; 37: e296 https://doi.org/10.3346/jkms.2022.37.e296 PMid:36254532 PMCid:PMC9577356 |
||||
| 4.Whittaker M, Rodrigues S, Cooke G, Berangere V, Donelly CA, Ward H, et al. How COVID-19 affected academic publishing: A 3-year study of 17 million research papers. Int J Epidemiol 2025; 54: dyaf058. https://doi.org/10.1093/ije/dyaf058 PMid:40421615 PMCid:PMC12107239 |
||||
| 5.Brandt MD, Ghozy SA, Kallmes DF, McDonald RJ, Kadirvel RD. Comparison of citation rates between COVID and nonCOVID articles across 24 major scientific journals. PloSONE 2022; 17: e0271071 https://doi.org/10.1371/journal.pone.0271071 PMid:35895698 PMCid:PMC9328554 |
||||
| 6.McGuire DK, Marx N, Deanfield JE, Inzucchi SE, Pop-Busui R, Mann JFE, eta l. Oral semaglutide and cardiovascular outcomes in high-risk type 2 diabetes. New Engl J Med 2025; 392:2001-12. https://doi.org/10.1056/NEJMoa2501006 PMid:40162642 |
||||
| 7.Laffin LJ, Kopjar B, Melgaard C, Wolski K, Ibbitson J, Bhikam S, et al. Lorundrastat efficacy and safety in uncontrolled hypertension. New Engl J Med 2025; 392: 1813-23. https://doi.org/10.1056/NEJMoa2501440 PMid:40267417 |
||||
| 8. Humbert M, Mclauglin VV, Badeh DB, Gibbs SR, Gomberg-Maitland M, Preston IR, et al. New Sotatercept in patients with pulmonary hypertension at high risk for death. New Engl J Med 2025; 392: 1987-2000. https://doi.org/10.1056/NEJMoa2415160 PMid:40167274 |
||||
| 9. Karr S, MAkkar RR, Whiusenant BK, Hamid N, Naik H, Tadros P, et al. Two-year outcomes of tarnscatheter edge-to edge repair for sever tricuspid regurgitation: The TRILUMINATE Pivotal RandomisedControlled trail. Circulation 2025; doi: 10.1161/CIRCULATIONAHA.125.074536 https://doi.org/10.1161/CIRCULATIONAHA.125.074536 PMid:40159089 |
||||
| 10. Choi KH, Park H, Lee JY, Jeong JO, Kim CJ, Yun KH., eta l. Efficacy and safety of clopidogrel versus aspirin monotherapy in patients at high risk of subsequent cardiovascular event after percutaneous coronary intervention (SMART CHOICE 3): a randomized open-label multicenter trial. Lancet 2025; 405: 1252-63. https://doi.org/10.1016/S0140-6736(25)00449-0 PMid:40174599 |
||||
| 11.Nichols SJ, Neslon AJ, Ditmarsch M, Kastelein JJP, Ray KK, Navar AM, et al. Safety and Efficacy of Obicetrapib in patienst with high cardiovascular risk. New Engl J Med 2025; doi: 10.1056/NEJMoa2415820 https://doi.org/10.1056/NEJMoa2415820 PMid:40337982 |
||||
| 12. Rao SV, O'Donaghue ML, Ruel M, Rab T, Tamis-Holland J, Alexander JH, et al. 2025 ACC/AHA/ACEPT/NAEMSP/SCAI guideline for management of patients with acute coronary syndromes: A report of the American College of Cardiology/ American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2025; 151: e00-e00. Doi: 10.1161/CIR.000000000001309. https://doi.org/10.1161/CIR.0000000000001309 |
||||
| 13.Arya A, Di Biase L, Bazan V, Berruezo A, d'Avila A, Della Bella P , et al. Epicardial ventricular arrhythmia ablation: a clinical consensus statement of the European Heart Rhythm Association of the European Society of Cardiology and the Heart Rhythm Society, the Asian Pacific Heart Rhythm Society, the Latin American Heart Rhythm Society, and the Canadian Heart Rhythm Society. Europace 2025; 27: euaf055. Doi: 10.1093/europace/euaf055 https://doi.org/10.1093/europace/euaf055 PMid:40163515 PMCid:PMC11956854 |
||||
| 14. Deharo JC, Dreyfus J, Bongiorni MC, Burri H, Defaye P, Glikson M, et al. Management of patients with transvalvular right ventricular leads undergoing transcatheter tricuspid valve interventions: a scientific statement of the European Heart Rhythm Association and the European Association of Percutaneous Cardiovascular Interventions of the ESC endorsed by the Heart Rhythm Society, the Asian Pacific Heart Rhythm Society and the Canadian Heart Rhythm Society. Europace 2025; 27: euaf061. Doi: 10.1093/europace/euaf061 https://doi.org/10.1093/europace/euaf061 PMid:40163675 PMCid:PMC12077151 |
||||
| 15. Merino JL, Tamargo J, Blomström- Lundqvist C, Giuseppe Boriani G, Crijns HJGM, Dobrev D, et al. Practical Compendium of Antiarrhythmic Drugs: A Clinical Consensus Statement of the European Heart Rhythm Association of the ESC | ||||
| 16. Glikson M, Burri H, Abdin A, Cano O, Curila K, Pooter J, et al. European Society of Cardiology (ESC) clinical consensus statement on indications for conduction system pacing, with special contribution of the European Heart Rhythm Association of the ESC and endorsed by the Asia Pacific Heart Rhythm Society, the Canadian Heart Rhythm Society, the Heart Rhythm Society, and the Latin American Heart Rhythm Society. Europace 2025; 27: euaf050 Doi: 10.1093/europace/euaf050 https://doi.org/10.1093/europace/euaf050 PMid:40159278 PMCid:PMC11957271 |
||||
| 17.Svennberg E, Han JK, Caiani EG, Engelhardt S, Ernst E, Paul Friedman P, et al. State of the Art of Artificial Intelligence in Clinical Electrophysiology in 2025: A Scientific Statement of the European Heart Rhythm Association (EHRA) of the ESC, the Heart Rhythm Society (HRS), and the ESC Working Group on E-Cardiology. Europace 2025; 27: euaf071 doi: 10.1093/europace/euaf071 https://doi.org/10.1093/europace/euaf071 PMid:40163651 PMCid:PMC12123071 |
||||
| 18. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for | ||||
| the evaluation and management of chronic kidney disease. Kidney Int 2024; 105: S117-S314. https://doi.org/10.1016/j.kint.2023.10.018 PMid:38490803 |
||||
| 19.CDC. COVID-19. Available at: URL: https:// www.cdc.gov/covid | ||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
