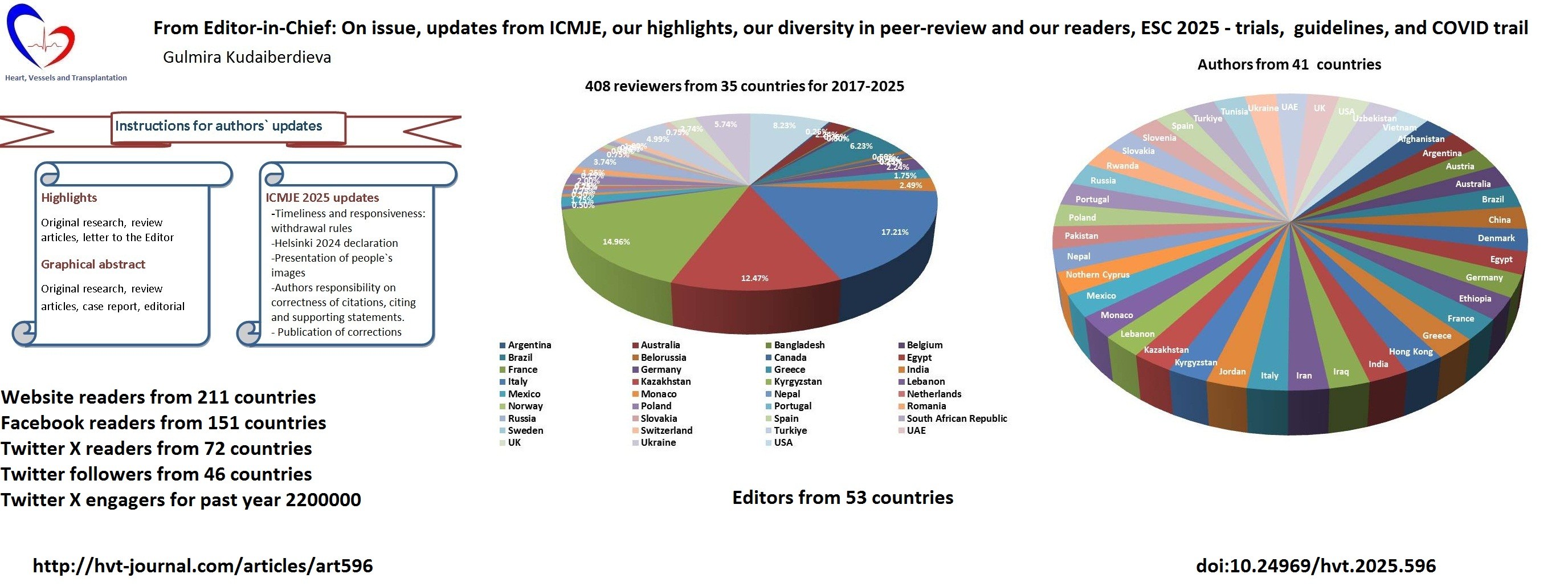
From Editor-in-Chief: On issue, updates from ICMJE, our highlights, our diversity in peer-review and our readers, ESC 2025 - trials, guidelines, and COVID trail
EDITORIALS
From Editor-in-Chief: On issue, updates from ICMJE, our highlights, our diversity in peer-review and our readers, ESC 2025 - trials, guidelines, and COVID trail
Article Summary
- DOI: 10.24969/hvt.2025.596
- CARDIOVASCULAR DISEASES
- Published: 13/09/2025
- Received: 07/09/2025
- Accepted: 08/09/2025
- Views: 2990
- Downloads: 2344
- Keywords: Biomedical publishing, guidelines, trials, cardiovascular medicine, surgery, transplantation, internal medicine, public health
Address for Correspondence: Gulmira Kudaiberdieva, Editor-in-Chief, Heart, Vessels and Transplantation
E-mail: editor@hvt-journal.com
ORCID: 0000-0002-4794-8435, 0000-0003-4099-8816 Scopus ID: 7003985934
Editorial

Graphical abstract
Key words: Biomedical publishing, guidelines, trials, cardiovascular medicine, surgery, transplantation, internal medicine, public health
The good book is never finished
It goes on whispering to you from the wall
Virginia Wolf
Dear Readers,
In this September 2025 issue of the journal, we published selected during our peer-review articles of interest for you: original research articles on coronary anatomy and interventions, describing clinical course and outcomes of percutaneous coronary interventions (PCI) in patients with coronary ecstasies, as well as protection of PCI-related injury with ranolazine; articles on vascular disease surgery- pathologic-anatomical features of aortic aneurysms and as well vascular repair and reconstruction of lower limb sarcoma cases; article on general surgery – outcomes of retropubic versus transvesical adenectomy in benign hyperplasia; articles on pediatric care- analysis of association of perinatal mortality with birth weight, experience of allergy tests in diagnosis of allergic diseases and asthma in children, clinical manifestations and outcomes of surgery for congenital high intestinal obstruction In newborns, often also associated with cardiac congenital defects; outcomes of unloading strategies in severe COVID patients treated with extracorporeal membrane oxygenation. Two review articles of interest for a wide audience and public health: nutritional value of yak milk and trends on adolescent health. We have 3 case reports on rare and complicated diseases or manifestations: multimodality imaging of congenital absence of pericardium; imaging in rare case of Balo`s concentric sclerosis developed after viral infection with importance for neurovascular branch as well for presentation and differential diagnosis and finally the multidisciplinary management of Staphylococci infective endocarditis presented as dengue fever. We have historical note in this issue on outstanding physician who was a general, who took part in a war for independence and politician, but also well known as physician who inoculated smallpox in Boston (type of vaccination) and was a first obstetrician gynecologist who took care of pregnant woman during pregnancy an delivery, the work usually carried by midwifes in 18th century. We have interesting letters discussing the new robust evidence presented in article published in June 2025 issue on relation between extent of coronary artery disease and obstructive sleep apnea and gaps in knowledge on the topic. We have also an editorial, prepared by Invited expert discussing the strength and weakness, gaps in knowledge and directions for research of knowledge presented in article on risk factors of coronary artery disease in patients with chronic kidney disease. Our editors with their colleagues prepared several editorials to attract you attention to the new guidelines and consensus guiding documents that provide recommendations for you, so you implement in your clinical practice: what is new in ACC/ AHA 2025 guidelines on acute coronary syndromes and comparison with ESC guidelines; updates form consensus document on conduction system pacing presented at EHRA 2025 on indications, implantation techniques, follow-up and management of patients with pacemakers; documents on how to perform ultrasound- guided vascular cannulation (venous or arterial lines, vascular access etc.) and multimodality imaging in management of patients with left ventricular assisted devices.
I would like also to share that recently (in April 2025) ICMJE updated its previous version (1). The major update for all is that organization ceased publication of journals following the rules of ICMJE, we were also on that list. The main reason behind this decision of ICMJE Editors was increase in number of predatory journals that ICMJE (2) and organization cannot check or regulate as trusted sources all journals who state they follow rules of ICMJE, while in fact not. In their Editorial (2), ICMJE Editors they defined the predatory journals and how to recognize them. Similarly, we published the Editorial prepared by our Editor Giuseppe Biondi -Zoccai and his colleagues on predatory journals, as number of requests to our authors to submit to their in fact dishonest journals for money has increased as well (3).
In addition several amendments to ICMJE rules (1) have been done:
-Timeliness and responsiveness of Editorial offices and Editors to authors queries, including if withdrawal. Authors could consider article withdrawn if they did not receive response from Editors;
- Diversity and inclusion – on presenting images of people, that people should be treated with dignity, respect and solidarity, consider publication of people photos only if necessary;
- Ethics in human studies statements: access and use updated Declaration Helsinki 2024 available at: URL: www.wma-net/policies-post/wma-declaration-of-helsiinki;
- Corrections - there are several updates on publication of corrections, and one of them that ICMJE recommends for studies published 10 years ago, to assess whether evidence and science presented are still important in nowadays as there is a constant progress in scientific evidence, authors may not be available and if not, the error may not need correction;
-Citations - Authors now are responsible for citing references accurately and they should be cited in the text correctly and support statements.
We also would like to inform our readers on update of our instructions for authors: we now require in addition to graphical abstract, to provide highlights in a box, reflecting main results and key message from you research and/or review article, letter to the editor. Graphical abstract is required for original research, review article, case report, and editorial.
Our diversity of authors, reviewers and editors has increased over the years – 2017-2025. We have now reviewers from 35 countries (Fig. 1) and you can see increasing trend in the number external reviewers and their countries – from 18 reviewers for first issues in 2017 to 74 in 2023, 71 in 2024 and 57 for the first 3 issues in 2025 (Fig. 2). We have overall 408 reviewers. We received manuscripts for consideration for publication from authors from 41 countries (Fig. 3).
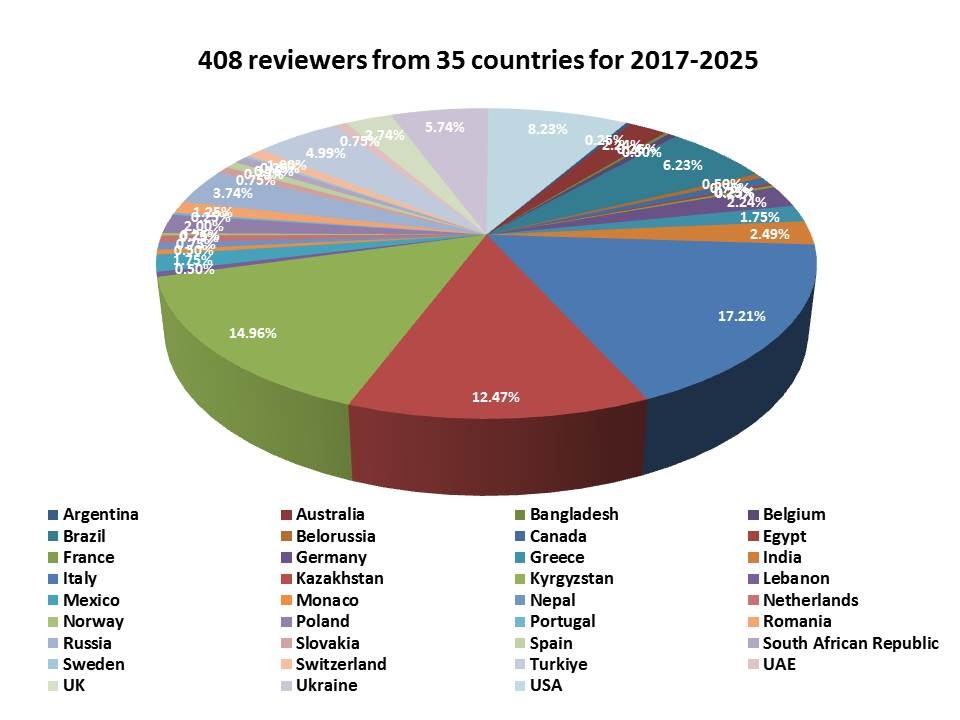
Figure 1. Our reviewers and their countries for a period of 2017-2025
We exercise a mixed model of peer-review, where editors not only execute, but also participate in peer-review and we have now Editors from 53 countries. All reviewers, editors and if there is a recommendation to revise or accept - authors as a part of peer-review process work hard to prepare articles for publication of high-quality that meet international contemporary standards.
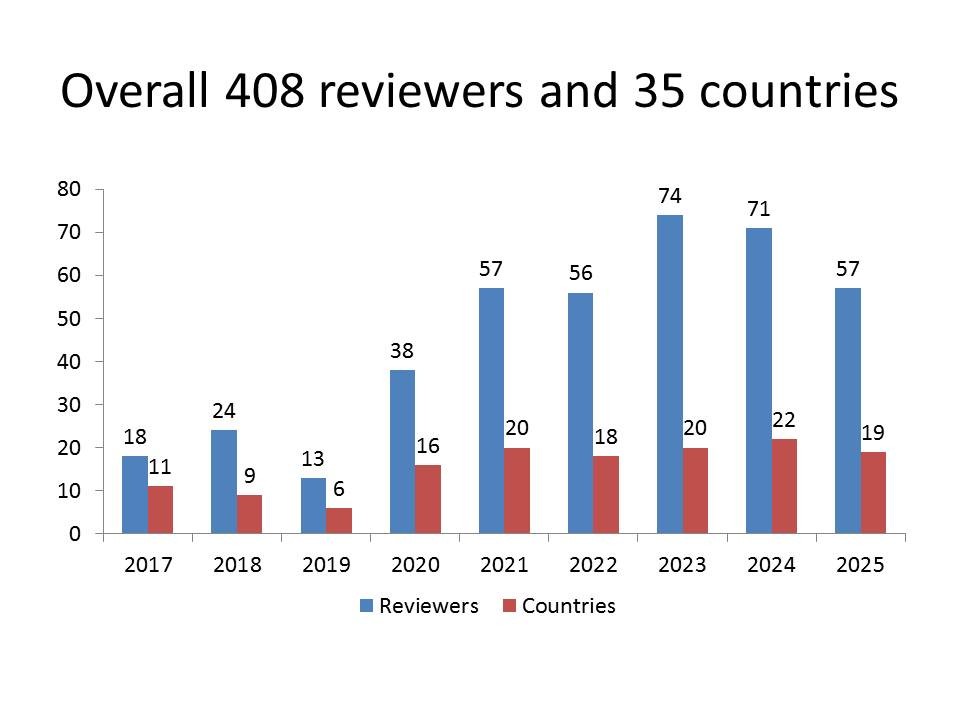
Figure 2. Time distribution of reviewers and their countries over a period 2017-2025

Figure 3. Countries of authors of manuscripts submitted for consideration for publication 2017-2025
Our readers on website are from 211 countries, friends and followers and all on social media reached our website using Facebook channel from 151 countries and Twitter X channel from 72 countries (Google, Facebook and Twitter analytics reports). We have now followers from 46 countries on twitter X, that make our articles tweets and accesses reach 2200 000 people around the world (Fig. 4 ). You can see live map our followers on website.

Figure 4. Engagers on Twitter X in June 2025
We have increase in countries and readers that access of our website using artificial intelligence (A.I.) like ChatGPT, A.I. that are being used for preparation manuscripts, graphs and figure, etc.
We will make analysis on whether there is a correlation between A.I. access of our articles and number of citation in future.
Analytic tools provided by technology empowers us as Editors as we see where our journal is being read, what topics are of importance for different regions of the world – website analytics gives us in details countries, region, cities and languages for each article, see example for research article in Figure 5, not only overall. We are working on linking each article to its readers geography map.
Now we are happy that Facebook also included in analytics not only how many viewed or reached, engaged but also top 10 countries of readers– see example in Figure 6.
ESC 2025 congress of cardiology took place in Madrid few days ago. Four major guidelines were presented: on myocarditis and pericarditis, management of dyslipidemias, valvular heart diseases, pregnancy and cardiovascular diseases (CVD), as well as consensus document on mental health in CVD (4-8). Our editors and invited experts are in preparation of editorials where they highlight new recommendations.
I would like to mention briefly the changes in recommendations on high blood pressure (BP) AHA/ACC 2025 guideline (9).
Though we are in preparation of comparison with ESC guideline on high blood pressure.
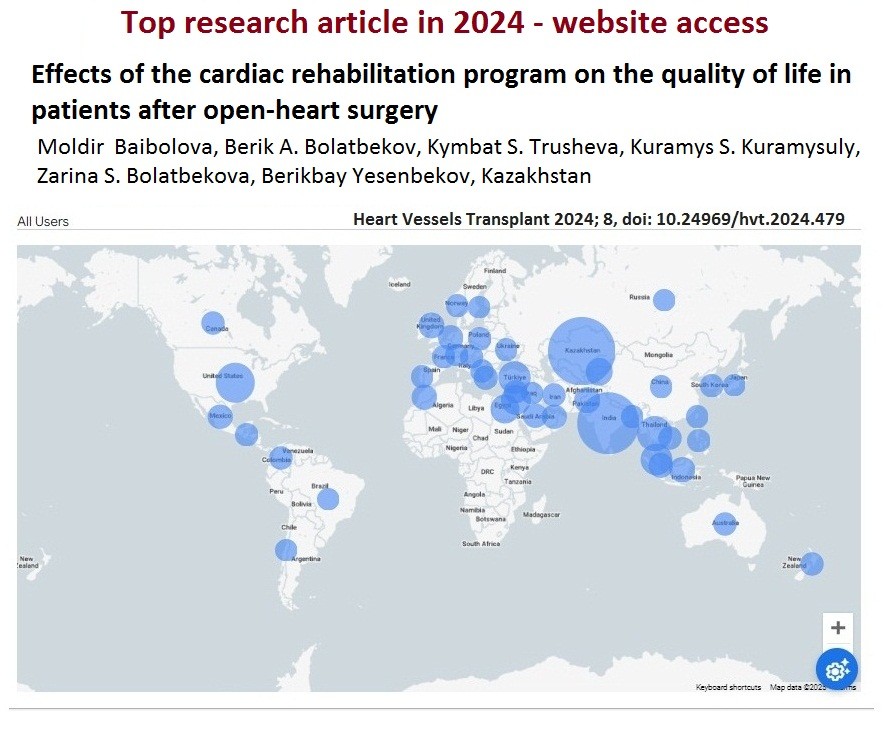
Figure 5. Countries of readers that accessed of our article open website – the most read article in 2024 (Google analytics)
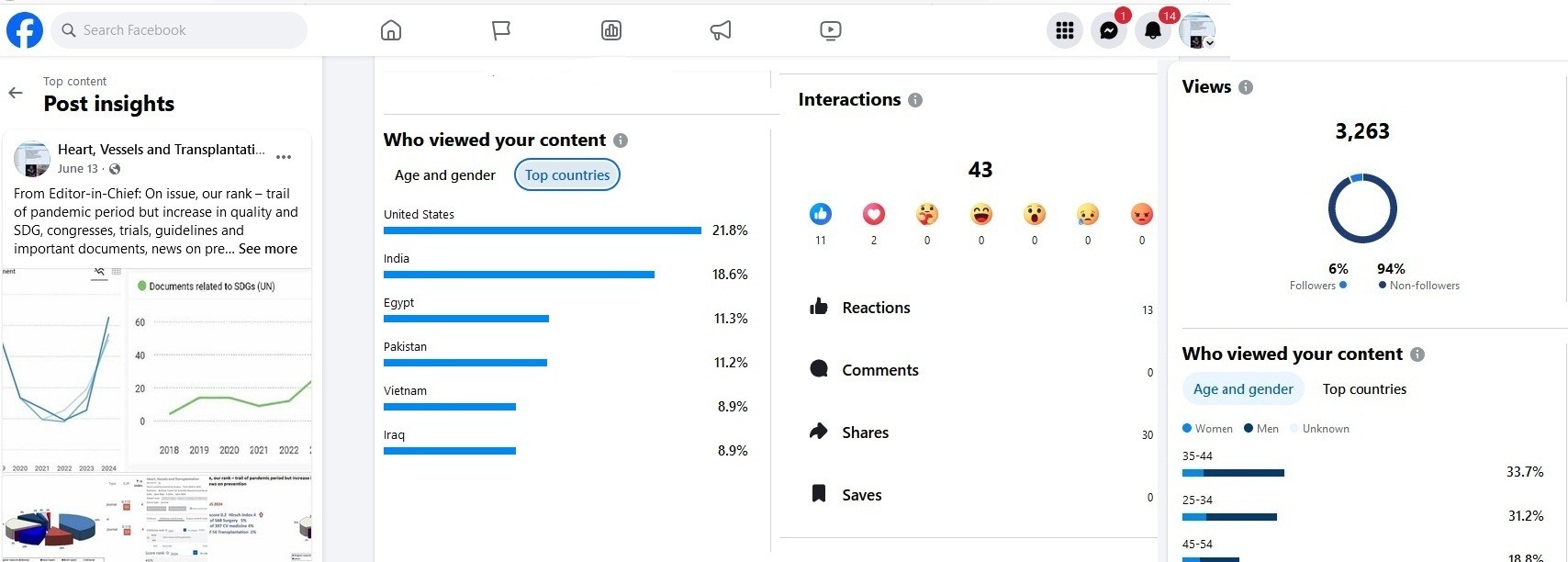
Figure 6. Top Facebook post in June 2005, with top 5 countries of readers, number interactions and number of views by followers and non-followers, demographics data of readers (Facebook analytics)
The 2025 AHA/ACC guidelines (9) introduces new terminology – severe hypertension is recommended to use instead of hypertensive emergency.
Secondary hypertension: screening for primary aldosteronism is recommended regardless of hypokalemia in cases or resistant hypertension to establish diagnosis and initiate early management. In patients with suspicion of primary aldosteronism it is recommended not to withhold antihypertensive treatment other than mineralcorticoid receptor antagonists (MRA) prior to initial screening in order not to delay screening procedures.
There are several revisions on initiation of BP lowering therapy and risk modification concerning use of different risk score, detailed diseases or change in BP threshold. In patients with hypertension with no clinical CVD and with diabetes and/or chronic kidney disease (CKD) and 10-year risk ≥7.5% (PREVENT study) the antihypertensive treatment is recommended to initiate when systolic blood pressure (SBP) ≥130 and diastolic blood pressure (DBP) ≥80 mm Hg to reduce CVD risk and mortality. In patients without CVD disease and 10-year risk (PREVENT) <7.5% it is recommended to initiate BP lowering if SBP≥130 and DBP≥80 mm Hg levels remain after 3-6 month of lifestyle modification to prevent target organ damage and mitigate further raise in BP.
For patients with hypertension and diabetes, angiotensin-converting enzyme inhibitor (ACEI), angiotensin receptor blocker (ARB) use was class of recommendations (COR) 2 in presence of albuminuria. Now it is revised as ACEI or ARB are recommended (COR 1) in patients with estimated glomerular filtration rate (eGFR) levels <60 ml/min/1.73m2 and albuminuria of ≥30 mg/g or should be considered (COR 2a) when mild albuminuria (<30 mg/g) is present to prevent diabetic kidney disease development. The changes are detailed levels of eGFR, albuminuria and COR.
For patients with hypertension and CKD, ACEI was class 2b and ARB - class 2a recommendations to start BP lowering therapy. New recommendation is - either ACEI or ARB (not both) are recommended (COR 1) for patients with hypertension and CKD (eGFR<60 ml/min/1.73m2) and albuminuria (≥30 mg/g) to prevent CVD risk and delay progression of CKD.
There are new recommendation for patients with intracerebral hemorrhage (ICH) and ischemic stroke. For patients with acute ICH with SBP 150-220 mm Hg lowering of BP to 130 - <140 mmHG for at least 7 days is beneficial, but stop antihypertensive if less than 130 mmHg to improve functional outcomes. For patients with ischemic stroke undergoing endovascular brain reperfusion lowering of BP less 140 mmHg during first 24-72 hours is harmful.
For BP lowering therapy in hypertension to prevent mild cognitive dysfunction and dementia (2a), threshold <130mm Hg is recommended (COR 1).
There are several new recommendations for pregnant women with high BP. The revision is about the BP lowering drugs that harm increased. Now, not only direct renin inhibitors and ACEI, but also ARB, MRA, atenolol and nitroprusside are contraindicated in pregnancy. New antihypertensive medications are recommended to reduce adverse events in pregnant women if BP ≥160/110 mmHg documented by repeated measurement of 15 minutes apart, The goal is to reduce BP less 160/110 mmHg within 30-60 minutes. In pregnant with BP 140-159/90-109 mm/Hg prior to 20 weeks gestation, BP lowering therapy is recommended to decrease it to <140/90 mmHg to reduce the maternal and perinatal mortality.
New COR 1 recommendation is patients with resistant hypertension and renal denervation - multidisciplinary team evaluation and management are recommended, the benefit and risk of procedure or medical therapy should be discussed with a patient to help him her choose therapy.
New expert panel document (10) was released recently to the attention of our arrhythmia specialists on the use of pentaspline pulsed field ablation (PFA) system in atrial fibrillation (AF) ablation procedures. Pulse field ablation system is nonthermal ablation fluoroscopy based system. Not all laboratories have 3-dimensional mapping capabilities and fluoroscopy remains the viable option. In this document experts shared their recommendation on indications, techniques of pentaspline PFA for AF ablation.
There are few trials presented at ESC 2025 congress that caught my attention (11). In BEAT-PAROX-AF randomized controlled trial (RCT) Jais P, et al. from France showed that PFA and radiofrequency ablation (RFA) of drug resistant paroxysmal AF had similar efficacy (77.2 vs 77.7% at one year without AF) AF, but single-shot PFA versus pulmonary vein ablation RFA according to CLOSE protocol was associated with less duration of procedure and twice less procedural complications– 3.4% vs 7.6%. Thus PFA is feasible with similar efficacy and in those centers without access to mapping and use of only X-Ray seems good option in terms safety.
CUVIA PRR trial demonstrated the digital twin guided ablation of additional sites in atrium in addition to pulmonary vein isolation in persistent AF was associated with reduction of arrhythmia recurrence at 18 month by 48% (HR 0.52, 95% CI –0.33-0.82, p=0.004) (Kim D et al., South Korea).
OPINION trial showed that in patients undergoing valvular surgery at high risk of stroke with no AF, surgical left atrial appendage (LAA) occlusion did not reduce number of stroke events, transient ischemic attack and cardiovascular mortality at 1 –year (Wang Y, et al. China). Thus, LAA occlusion in absence of arrhythmia in such category of patients is not warranted.
Another negative result trial is REFINE –ICD (Exner D et al. Canada) showed that prophylactic ICD therapy in patients with prior myocardial infarction (MI) (>2 months) and moderate left ventricular (LV) dysfunction (ejection fraction, EF -36-50%) and abnormal T wave alternance and heart turbulence had no benefit in reduction of 5.7 years all-cause mortality, sudden cardiac death and cardiac mortality. Key behind no effect is probably a moderate LV dysfunction.
NEWTON-CABG Cardiolink-5 established no benefit of moderate –high intensity statin (evolocumab) therapy in prevention of saphenous vein graft failure at 2 years after coronary artery bypass surgery (Verma S, et al. Canada).
Finally, analysis of 2 trails BETAMI and DANBLOCK demonstrated that beta-blockers reduce composite outcome (all-cause mortality, new MI, revascularization, ischemic stroke, heart failure (HF) and malignant ventricular arrhythmia) by 15% (HR 0.85 95%CI 0.75-0.98 p=0.027( i n patients with MI and without HF (EF>40%) (Dan Atar, Norway). Similarly meta-analysis of REBOOT, BETAMI ,DANBLOCK, and CAPITAL_RCT trials (Rosella X, Spain) revealed that beta-blockers in patients with moderately reduced (EF 40-49%) reduced all cause death, new MI and HF by 25% at 1 year r (HR 0.75 CI 0.58-0.97 p=0.031).
DANCAVAS 2 trials showed not benefit of comprehensive CVD screening (ECG gated computed tomography coronary calcium score, aortic iliac aneurysm screening, AF, ankle-brachial index (peripheral artery disease), and blood pressure level (hypertension) HbA1c (diabetes) and lipid tests) among 60-64 years old male in terms death from any cause during 7 years of follow-up. It is a rather expensive screening approach, more studies are needed.
Regarding COVID, new updated vaccines are approved for fall for individuals at high risk of severe diseases, though professional societies provide slightly different recommendations (12).
We would like to congratulate Professor Barbara Casadei with appointment as an Editor-in-Chief of JAMA Cardiology and wish our colleague (we know her from ESC leading positions and activities she led) all success and wonderful achievements.
Gulmira Kudaiberdieva
Editor-in-Chief
Heart, Vessels and Transplantation
Peer-review: Internal
Conflict of interest: None to declare
Authorship: G.K.
Acknowledgements and funding: None to declare
Statement on A.I.-assisted technologies use: We declare that we did not use AI-assisted technologies in preparation of this manuscript
Data and material availability: Does not apply
.
References
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
