Current trends of preparation of medical specialists at the remote industrial facilities in the Kyrgyz Republic
REVIEW
Current trends of preparation of medical specialists at the remote industrial facilities in the Kyrgyz Republic
Article Summary
- DOI: 10.24969/hvt.2026.627
- CARDIOVASCULAR DISEASES
- Published: 26/02/2026
- Received: 05/12/2025
- Revised: 10/02/2026
- Accepted: 11/02/2026
- Views: 957
- Downloads: 869
- Keywords: Public health, remote healthcare, mountain medicine, mountain rescue, medical education, acute mountain sickness, basic life support
Address for Correspondence: Aibek A. Ashyrbaev, Adam University, Bishkek, Kyrgyz Republic
Email: aibeka@mail.ru
ORCID: Aibek A. Ashyrbaev - 0000-0001-9902-2346; Svetlana R. Sirmbard - 0009-0009-1235-5371
Aibek A. Ashyrbaev, Svetlana R. Sirmbard
Adam University, Bishkek, Kyrgyz Republic
Abstract
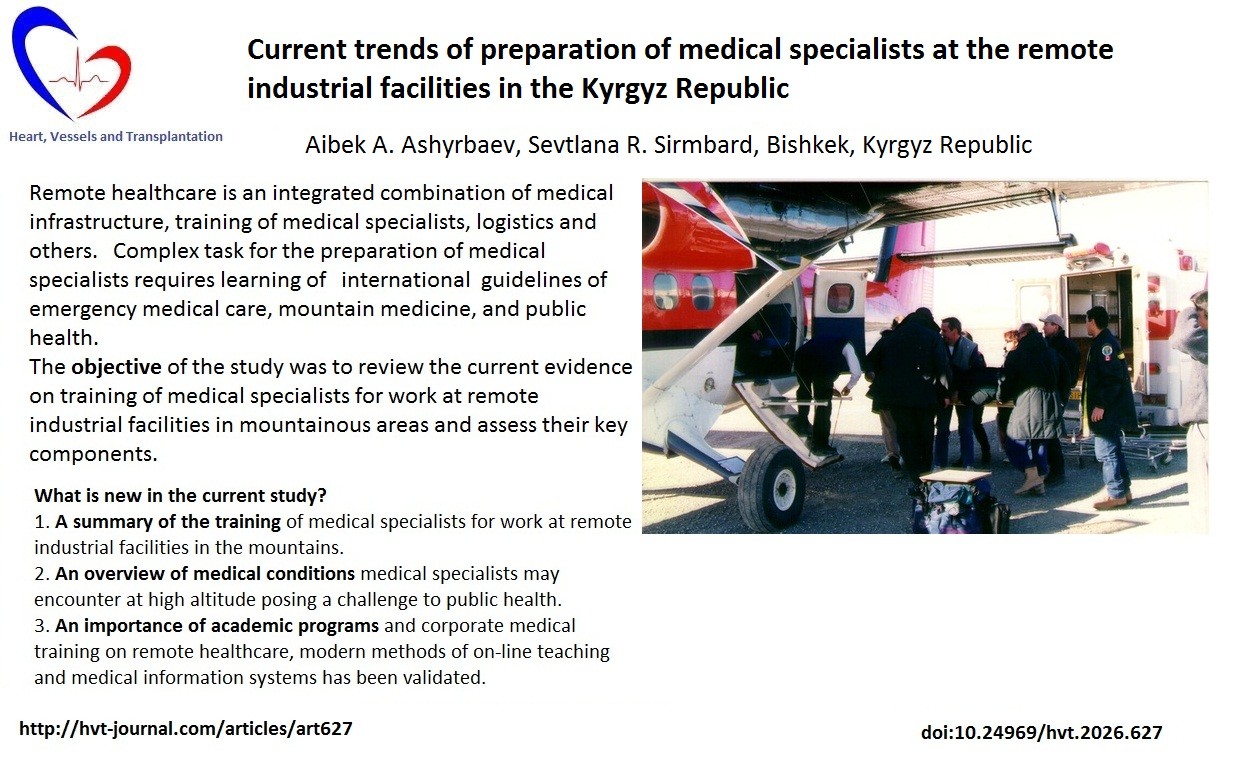
Objective: Remote healthcare (RH) is currently an important area in practical medicine. Improving and maintaining the health of the population in remote areas is a priority of the state. To achieve this goal, the training of medical personnel at remote industrial facilities (RIF) is crucial. The preparation of medical specialists (MS) for work at RIF in the mountainous areas in Kyrgyz Republic is lacking. The objective of the study was to review the current evidence on training of MS for work at remote industrial facilities in mountainous areas and assess their key components.
Methods: The literature search was done in electronic databases: PubMed, Elibrary and websites of medical journals (High Altitude Medicine and Biology, Journal of Travel Medicine), and organizations - International Commission For Alpine Rescue Medical Commission. Overall, 75 articles were identified initially, 20 articles met inclusion criteria.
Results: RH is a complex system for organizing medical care in areas located far away from populated areas. The British system for training medical personnel for remote locations served as a pattern to the further development of similar programs in other countries. There are various types of courses regarding RH in the world. Current trends of preparation of MS at the RIF include practical learning of algorithms of American Heart Association and other international guidelines. Online teaching methods are widely used for training MS. There are other various types of courses regarding RH on demand. The Siberian State Medical University allied with the Center for Corporate Medicine Group of Companies in Tomsk city, are leaders in RH in the Russian Federation. In the Kyrgyz Republic, there is no special program for RH. MS working at remote industrial sites in the mountains have to study a standard course of emergency medicine. It is crucial to develop a special remote medicine course for the preparation of medical staff for RIF in Kyrgyz Republic.
Conclusion: Remote healthcare is a complex task demanding special training of a medical specialist for work in remote areas, building infrastructure, logistics, legal aspects. Mountain medicine is a part of RH and it poses a challenge to public health. Common medical problems at RIF in the mountains are acute mountain sickness, high altitude pulmonary edema, hypothermia, and traumas that require immediate treatment and evacuation. MS must have professional competencies, leadership, communication, and professional skills in emergency care, mountain medicine, infection control, occupational medicine etc. There is a big need to upgrade the skills of MS in RH in the Kyrgyz Republic to international standards.
Key words: Public health, remote healthcare, mountain medicine, mountain rescue, medical education, acute mountain sickness, basic life support
Introduction
In recent years, there is a growing interest on the topic of "remote healthcare." This encompasses a wide range of issues related to medical support at remote industrial facilities (RIF), such as training of medical specialists, creation of medical infrastructure, logistics and communications, the implementation of treatment and preventive measures, and other issues. Originating in the UK in the mid-1960s, the "remote healthcare" system has been continuously refined over decades and has proven successful in the North Sea, the Arctic, and oilfields of the Middle East.
Remote healthcare (RH) is a comprehensive system of the organization of the medical care in remote areas located at significant distances from populated areas where administrative, economic, social, medical infrastructure and communications are well-developed (1).
Graphical abstract
Developing industrial RH requires comprehensive approaches, including training of the medical specialists, clinical medicine, management, logistics, economics, and law. The industrial RH system has evolved over time. Medical experts from various countries have developed training programs for medical specialists on remote sites, but there is still no consensus on the content of medical training or uniform international certification (2).
Educational standards exist for all medical specialties in the Kyrgyz Republic. However the training of medical professionals working at remote sites is lacking. Usually, various kinds of doctors with insufficient training in emergency medicine are working at many RIF in mountainous areas of the Kyrgyz Republic.
The objective of the study was to review the current evidence on training of medical specialists for work at remote industrial facilities in mountainous areas and assess their key components.
Methods
Articles related to the training of medical specialists for RIF are very scarce. To conduct this study, an analysis of the articles about current methods of training medical specialists at remote sites was done.
The literature search was comprised of sources from electronic databases (Fig. 1): PubMed, Elibrary and websites of medical journals (High Altitude Medicine and Biology, Extreme Medicine), and organizations - International Commission For Alpine Rescue Medical Commission (ICAR MEDCOM). A manual search among conference materials on remote healthcare was executed (https://remotehealthcare.ru). Search key words were as following: public health; remote healthcare, mountain medicine, mountain rescue, medical education, acute mountain sickness, basic life support.
The inclusion criteria of articles for the narrative review were publications from 2015 to 2025. The time frame of the database searches was from December 1 to December 31, 2025. Literary sources included articles and conference materials related to current methods of training of medical specialists working at RIF in various geographic regions. The exclusion criteria of articles were articles without full text, duplicate publications, articles without relevant content or outcome.
The data search collected 75 articles and abstracts. Of 55 articles remained after initial screening for compliance with the aim of the research. Then five duplicate articles were removed, 25 articles were removed because full text was not available, and five articles were removed due to irrelevant content. Thus, 20 articles were selected for further analysis. Abstraction, synthesis, and analysis methods were used for the review. The study design is presented in Figure 1.
|
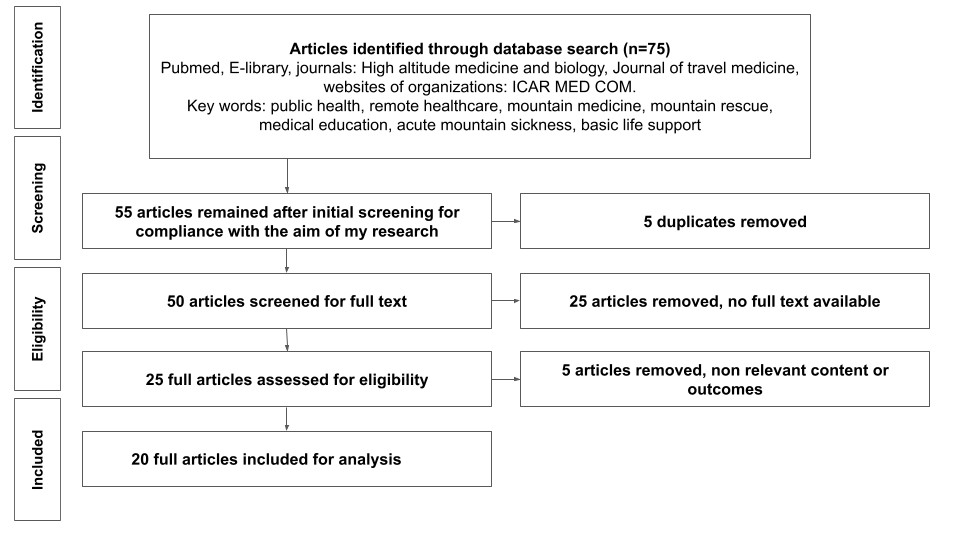
Figure 1. Study flowchart
Overview of high-altitude RIF in the world and associated medical conditions
The work at remote industrial sites in the mountainous regions is a special form of the organization of the labor in which shift workers are deployed for a limited period of time to industrial sites located in mountainous regions, sometimes at high altitudes. This working schedule significantly affects the health of shift workers. The Table 1 shows some examples of remote industrial sites located in mountainous regions of the Kyrgyz Republic and in the world.
|
Table 1. Examples of remote industrial sites located in mountainous regions of the Kyrgyz Republic and in the world |
|||
|
N
|
Name of the project, country |
Altitude (meters above sea level) |
Type of mineral resources |
|
1. |
Kumtor, Kyrgyz Republic |
3800-4200 |
gold |
|
2. |
Jerooy, Kyrgyz Republic |
3000-3500 |
gold |
|
3. |
Bozymchak, Kyrgyz Republic |
2400-2700 |
copper |
|
4. |
Chaarat, Kyrgyz Republic |
2400-2600 |
gold |
|
5. |
Morrococha, Peru |
4550 |
gold |
|
6. |
Serra de Pasco, Peru |
4330 |
polymetals |
|
7. |
El Indio, Chile |
3800-4000 |
polymetals |
|
8. |
Collahuasi, Chile |
4400-4600 |
copper |
|
9. |
Andina, Chile |
3400-4200 |
copper |
|
10. |
Climax, USA |
4350 |
molibden |
|
11. |
Summitville, USA |
4050 |
gold |
|
12. |
Potosi, Bolivia |
4830 |
polymetals |
|
13. |
China |
5228 |
solar electrical station |
|
14. |
Mauna Kea, Hawai |
4200 |
telescope |
Negative factors associated with shift work in mountainous areas include hypoxia combined with low barometric pressure, cold weather, constant wind, increased solar radiation, exposure to harmful industrial factors, living in a confined space, disruption of the work-and-rest schedule, diet, remoteness from social and medical infrastructure, limited medical resources, etc (3-10).
At altitudes above 3,500 meters, shift workers may develop specific pathological conditions such as acute mountain sickness, high-altitude pulmonary edema, and high-altitude cerebral edema. The Lake Louise Acute Mountain Sickness Questionnaire is used for the diagnosis of acute mountain sickness (AMS) (3, 4).
According to the literature, the incidence of AMS among mountain climbers varies from 12% to 70%. Such a wide range in data is due to many factors, e.g. an altitude, the speed of ascent, age, gender, etc. (5-7). The incidence of AMS among shift workers at an altitude of 4,000 m is about 25% (8).
High altitude have negative influence on the health of shift workers, such as increased fatigue, sleep disorders, exacerbation of chronic diseases, etc. Stress, depression, anxiety, and frustration are resulting from general hypoxia and low barometric pressure. As well, shift workers are exposed to adverse industrial factors such as air pollution, noise, vibration, and exposure to chemicals and traumas (9, 10).
Training of medical personnel to work in RIF
Training of medical personnel for work at remote sites has begun in the United Kingdom in 1978 (1). The educational programs for the training of medical specialist working in the North Sea offshore oil rigs have been developed. Medical training for the offshore projects primarily included Basic Life Support, Advanced Cardiac Life Support, Basic Off Shore Emergency Training, fundamentals of marine and diving medicine, food hygiene etc. The British system of training has been used for many years in the North Sea, Arctic, Antarctic and Middle East regions. Eventually British system was utilized as a pattern for similar programs in other parts of the world, such as Canada, Russia, China, Kazakhstan etc.
In the former USSR, medical specialists working at remote sites were involved with industrial operations at the Arctic region, Siberia, Sakhalin, Eastern part of Russia etc. However, there was no special “remote medicine” training. Emergency medical skills remained as the main attribute for medical specialists at remote sites. They had limited knowledge in the internal diseases, occupational health, hygiene, and epidemiology (11).
Nowadays, a medical specialist at the RIF must be proficient in emergency medicine, risk management, telemedicine, medical information systems and utilization of complex medical equipment.
Russian Federation has a huge territory and it is a leading country in the field of remote healthcare Logunov et al. (12) indicates that training of medical specialists for work at remote industrial sites should be an important part of the strategic development of any modern company conducting work at remote locations.
Sokolovich et al. (13) analyzed 75 Technical Assignments for the “Center for Corporate Medicine”, and he states that medical professionals at the RIF should have a wide range of competencies, a deep understanding of general medical issues, as well as Basic and Advanced Life Support training. Bygvraa et al. (14) believes that only knowledge in emergency medicine is not enough, there are differences in the training of medical staff depending on the remote site location. Doctors on offshore projects must have knowledge of maritime medicine, occupational pathology, tropical medicine, primary care, travel medicine, risk assessment and local legislative procedures (14).
Badmaeva et al. (15) emphasizes the importance of public health knowledge and regulatory framework, issues regarding telemedicine consultations with the “mainland”, and the importance of medical information system on remote sites (15). Orlov et al. (16) notes the shortage of personnel and the lack of specialized training for medical specialists in Russia's Arctic shelf zone. He recommends a multi-level training model, the introduction of general mandatory qualification requirements, on-line simulation training, and an introductory course for doctors before deployment to remote site.
Current academic programs on remote healthcare and mountain medicine
These days, medical specialists working in remote places must be proficient with telemedicine technologies, medical information systems and complex medical equipment.
Pittman et al. (17) launched a medical elective on wilderness medicine in the medical school. The goal is to introduce students into wilderness medicine. Upon completion of the 2-week course, students learn fundamental concepts of wilderness medicine, to identify and initiate treatment for common conditions in austere environment. Topics include trauma stabilization, patient transportation, AMS, high altitude pulmonary edema, hypothermia, frostbite, disaster response, high angle rescue, expedition medical kits etc.
There is a medical school teaching high altitude medicine in China (18). The school of high altitude medicine was established at the Third Military Medical University, Tibet. Students study high altitude medicine during internship at the general hospital for 3 months. On-site teaching method is an innovative approach for training in high altitude medicine (18).
In the Russian Federation, the RH program is under way in some leading medical universities. The Siberian State Medical University in Tomsk has developed two post-graduate programs on remote healthcare: a program for advanced training in remote medicine and a program for professional retraining (19). Modular approaches, provision of educational materials by means of various educational technologies in a hybrid format are currently used for the training of medical specialists in remote medicine. Medical specialists wishing to work in the remote medicine can choose one of two programs. The advanced training program provides training within their current qualifications, improving or acquiring new competencies necessary for professional work. The advanced training program in remote medicine is accredited by the State continuing medical education system. It is the first advanced training program in the Russian Federation. The length of the program is two weeks. Upon completion, students receive a Certificate of Advanced Training.
If medical specialist is going to choose a program for professional retraining, he acquires a new medical competencies necessary for a new professional activity. The program for professional retraining is a deeper program and it covers a broad range of required management competencies. The length of training is three and a half months. The required competencies in remote medicine include leadership, communication, and professional skills. Upon completion of the program, the medical specialist receives a Diploma of Professional Retraining (19).
Telemedicine for remote healthcare and mountain medicine
Over the last decade, the development of the information technologies has led to the development of telemedicine methods for the diagnosis and treatment of patients at the remote sites. Martinelli et al. (20) has described the increasing role of telemedicine consultations in the work of medical centers located in the mountains.
Telemedicine technologies are becoming an effective tool for increasing the availability of medical care in remote areas (20).
Podsiadlo et al. (21) has launched an e-learning platform on medical education for mountain rescuers concerning hypothermia. This course has increased the knowledge of hypothermia among mountain rescuers. E-learning platform became an effective instrument for the medical education of mountain rescuers (21).
Buono et al. (22) indicates that methods of telemedicine have been widely introduced into the training of medical specialists at remote sites. These methods allow creation of a flexible class schedule and the delivery of the classes anywhere, regardless of the instructor's location (22).
Corporate medical training of medical specialists working in RH
Center for Corporate Medicine (CCM) from Tomsk is providing training for medical specialists working at RIF according to Russian and international standards. Core activities include medical assistance, consulting services, and medical check-ups. The training program has four modules: organizational module, tactical module, clinical module, and logistics. Program includes learning of international emergency medicine protocols of the American Heart Association and American College of Surgeons (23).
Some companies operating at remote locations demand from medical specialist to follow the Guidelines of ICAR MEDCOM (3, 24) or obtain additional special trainings, e.g. Basic Off Shore Emergency Training (BOSET), Avalanche Rescue or Air Ambulance Rescue Training etc.
At some remote industrial sites medical evacuations of patients are done by helicopters (Air ambulance). Medical crew on air ambulance must have special training. In mountainous areas, medical evacuations are possible only with helicopter. For airplane, it is necessary to have runway on site, unlike helicopter, which can land on any terrain.
Grissom et al. (25) states that safety is a number 1 priority for any medical helicopter involved in rescue operation, which is considered at each decision point, so the medical helicopter crew is empowered to decline the mission for safety reasons at any step.
Tomazin et al. (26) indicates that the use of helicopter can significantly shorten rescue missions especially in mountainous areas. Rescue helicopters should work within the existing medical emergency system with appropriate mountain rescue and medically trained staff and with medical and rescue equipment on board. Figure 1 shows medical evacuation of the patient with trauma from the mine site at an altitude of 3800 m, Kyrgyz Republic.

Figure 1. Medical evacuation of the patient with trauma from the mine site at an altitude of 3800 m, Kyrgyz Republic
Based on the ICAR MEDCOM, Wilderness Medical Society Guidelines for the Prevention, Diagnosis and Treatment of Acute Mountain Sickness: 2024 Update; Basic Life Support, Guidelines of the American Heart Association and European Resuscitation Council guidelines (3, 24, 27-29), we can conclude that medical specialist have to possess following theoretical knowledge and practical skills presented in Table 2.
|
Table 2. Theoretical knowledge and skills for the medical specialists at remote industrial sites in mountainous areas |
|||
|
N
|
Competency section |
Necessary knowledge |
Practical skills |
|
1. |
Emergency medicine |
Algorithms of BLS, ACLS, shock, acute coronary syndrome, anaphylaxis etc. |
CPR, defibrillation, intubation of trachea, intravenous access and therapy, medical evacuation |
|
2. |
Traumatology |
Industrial injuries, fractures, burns, traumatic brain injury etc. |
Immobilization, bleeding control, primary surgical treatment of wounds, medical evacuation |
|
3. |
Mountain medicine |
Acute mountain sickness, high altitude pulmonary edema, high altitude cerebral edema, hypothermia, frostbite |
Oxygen therapy, treatment in the hyperbaric chamber, medical evacuation |
|
4. |
Disaster medicine |
Fundamentals of treatment of mass casualties, triage |
Triage, coordination, medical evacuation |
|
5. |
Infection control |
Fundamentals of sanitary and hygiene measures |
Screening, organizing isolation procedures, early prevention, prophylactic measures |
|
6. |
Occupational medicine |
Dust, noise, vibration, use of chemical substances in the processing of ore |
Screening, early prevention, early diagnosis |
|
ACLS – advanced cardiac life support, BLS – basic life support, CPR – cardiopulmonary resuscitation |
|||
In the Kyrgyz Republic, there are no organizations providing medical training according to the guidelines of the American Heart Association so far. As an option, mining companies invite certified instructors from other countries to provide courses. Sometime mining companies send their medical staff to the accredited training centers abroad.
Four years ago, “Center for Corporate Medicine” from the Russian Federation has opened a training center to teach students and general population Basic and Advanced Life Support under auspices of European Resuscitation Council in Kyrgyz Republic. After completion of the course, students obtain Basic Life Support Certificate from European Resuscitation Council.
In addition to medical aspects, the development of medical care system at the RIF includes the creation of First Aid trained group of workers. They are an important element of the overall safety of the mining company. A systematic training of first aiders is the key factor to improve emergency care during emergencies.
Mining companies need to employ medical specialists who have earned an expertise in RH. Medical specialists must be current with emergency protocols published by international organizations and local healthcare organizations: American Heart Association, European Resuscitation Council, International Commission For Alpine Rescue etc (27-29).
Study limitations
The present study is a narrative review, which determines some limitations. The result of the study relates primarily to the RIF (mining industry) in Kyrgyz Republic, which limits the possibility of their extrapolation to other remote industrial facilities, e.g. oilfields, offshore rigs, etc. in other countries.
The data obtained are showing current trends of preparation of medical specialists at the RIF. The study reflects the situation at a specific point in time. However, these trends may change over time when the development of medical education, digital technologies, and telemedicine will occur.
Study may be biased by the availability and quality of the available articles, because existing articles may give an incomplete picture of actual practice. Thus, the obtained results should be considered as a basis for further research.
Conclusion
Remote healthcare is a complex task demanding special training of the medical specialists to work in remote areas, building infrastructure, logistics, legal aspects. Mountain medicine is a part of remote healthcare posing a challenge to public health. Common medical problems at remote industrial sites in the mountains are acute mountain sickness, high altitude pulmonary edema, hypothermia, and traumas, which require immediate descent to a lower altitude. Medical specialists must have professional competencies, leadership, communication, and professional skills in emergency care, mountain medicine, fundamentals of disaster medicine, hygiene, occupational health etc. There is a big need to upgrade the skills of medical specialists in remote healthcare in the Kyrgyz Republic to international standards.
Peer-review: External and internal
Conflict of interest: None to declare
Authorship: A.A.A. and S.R.S. equally contributed to preparation of manuscript and fulfilled all authorship criteria
Acknowledgements and funding: None to declare
Statement on A.I.-assisted technologies use: We declare that we did not use AI-assisted technologies in preparation of this manuscript
Data and material availability: Does not apply
References
| 1.Norman N, Valentine MJ. History, development of the concept and research. In: Remote medicine. A textbook for trainee and established remote health care practitioners. Norman N, Valentine MJ, editors. World Scientific Publishing. UK Limited: 2020; pp.1-15. https://doi.org/10.1142/q0222 |
||||
| 2.Antipov SA, Karpov AB, Badmaeva ER. Industrial medicine and remote healthcare in Russia. In: Remote Medicine. A textbook for trainee and established remote health care practitioners. Norman N, Valentine MJ, editors. World Scientific Publishing UK Limited: 2020; pp.260-2. https://doi.org/10.1142/9781786347510_0012 |
||||
| 3.Luks A, Beidleman BA, Freer L, Grissom CK, Keyes LE, McIntosh SE, et al. Wilderness medical society clinical practice guidelines on the prevention and treatment of acute altitude illness: 2024 Update. Wilderness Environ Med 2024; 35 (1_Suppl): 2S-19S. https://doi.org/10.1016/j.wem.2023.05.013 PMid:37833187 |
||||
| 4.Roach RC, Hackett PH, Oelz O, Bartsch P, Luks AM, MacInnis MC, et al. Lake Louise AMS Score Consensus Committee. The 2018 Lake Louise Acute Mountain Sickness Score. High Alt Med Biol 2019; 19: 4-6. doi: 10.1089/ham.2017.0164 https://doi.org/10.1089/ham.2017.0164 PMid:29583031 PMCid:PMC6191821 |
||||
| 5.Bania S, Lama TA. High altitude illness among rapidly ascending pilgrims to Kailash Mansorovar. J Nepal Health Res Counc 2023; 20: 734-8. doi: 10.33314/jnhrc.v20i3.4040 https://doi.org/10.33314/jnhrc.v20i3.4040 PMid:36974866 |
||||
| 6.Hertig D, Lichtblau M, Furian M, Ulrich S, Mayer L. Acute high-altitude illnesses - definition, prophylaxis, therapy. Ther Umsch 2025; 82: 209-14. doi: 10.23785/TU.2025.06.007 | ||||
| 7.Horiuchi M, Endo J, Akatsuka S, Uno T, Jones TE. Prevalence of acute mountain sickness on Mount Fuji: A pilot study. J Travel Med 2016; 23; 1-5. doi: 10.1093/jtm/taw024 https://doi.org/10.1093/jtm/taw024 PMid:27147731 |
||||
| 8.Farias JG, Jimenez D, Osorio J, Zepeda AB, Figueroa CA, Pulgar VM. Acclimatization to chronic intermittent hypoxia in mine workers: a challenge to mountain medicine in Chile. Biol Res 2013; 46: 59-67. doi: 10.4067/S0716-97602013000100009 https://doi.org/10.4067/S0716-97602013000100009 PMid:23760416 |
||||
| 9.Dartey E, Monney I, Sarpong K, Kuffour C. Occupational health hazards among large-scale gold mineworkers in Ghana. Occup Dis Environ Med 2022; 10: 149-66. doi: 10.4236/odem.2022.103012 https://doi.org/10.4236/odem.2022.103012 |
||||
| 10.Dzhusupov KO, Colosio C, Tabibi R, Sulaimanova CT. Occupational health in mountainous Kyrgyzstan. Ann Glob Health 2015; 81: 530-7. Doi: 10.1016/j.aogh.2015.08.017 https://doi.org/10.1016/j.aogh.2015.08.017 PMid:26709285 |
||||
| 11.Soldatov EA, Mamaeva SA, Gerasimova AA. Medical support for the Antarctic expeditions. Voenno-Med Z 2022; 343: 73-82. DOI: 10.52424/00269050_2022_343_10_73 https://doi.org/10.52424/00269050_2022_343_10_73 |
||||
| 12.Logunov KV, Antipov SA, Lepetinsky IS. Industrial healthcare in the Russian Arctic - trends and experience of recent decades. Marine Med 2022; 8: 118-26. doi: 10.22328/2413-5747-2022-8-3-118-126 https://doi.org/10.22328/2413-5747-2022-8-3-118-126 |
||||
| 13.Sokolovich EG. Personnel of health centers at remote industrial sites. Abstracts of the V International Conference on Remote Healthcare. September 4-5, 2025. Tomsk. | ||||
| 14.Bygvraa DA, Adhikari TB, Charalambous G. Jensen OC. Maritime doctors' skills and competencies: A review for policy analysis. Maritime Tech Res 2019; 22:.40-51. Doi: 10.33175/mtr.2020.206375 https://doi.org/10.33175/mtr.2020.206375 |
||||
| 15.Badmaeva ER, Antipov SA. Training personnel for the remote healthcare system. Current requirements. Science and education in modern society. IV International Scientific-Practical Conference: MCNS "Science and Education". Penza. 2021, pp. 132-135. | ||||
| 16.Orlov OI, Mamonova EYu, Romanov MA, Kalinina MYu. Requiremnets for medical personnel providing medical care at stationery industrial facilities at Arctic shelf region of Russia. Med Extreme Situat 2025; doi: 10.47183/mes/2025-409 https://doi.org/10.47183/mes.2025-409 |
||||
| 17.Pittman MA, Slone T, Wilson M. Introduction to wilderness medicine-a medical school elective. J Educ Teach Emerg Med 2020; 5: C1-C120. DOI: 10.21980/J8B93X https://doi.org/10.5070/M551046555 PMid:37465594 PMCid:PMC10332540 |
||||
| 18.Luo Y, Luo R, Li W, Huang J, Zhou Q, Gao Y. High altitude medicine education in China: Exploring a new medical education reform. High Alt Med Biol 2012; 13: 57-9. DOI: 10.1089/ham.2011.1090 https://doi.org/10.1089/ham.2011.1090 PMid:22429234 |
||||
| 19.Boykov VA. The experience in developing and implementing additional professional programs for remote healthcare specialists. Proceedings of the V International Conference on Remote Healthcare. 4-5 September, 2025. Tomsk city. Available at: URL: https://remotehealthcare.ru | ||||
| 20.Martinelli M, Moroni D, Bastiani L, Mrakic-Sposta S, Giardini G, Pratali L. High-altitude mountain telemedicine. J Telemed Telecare 2022; 28: 135-45. doi: 10.1177/1357633X20921020 https://doi.org/10.1177/1357633X20921020 PMid:32539486 PMCid:PMC8915246 |
||||
| 21.Podsiadlo P, Kosinski S, Darocha T, Salapa K, Sanak T, Brugger H. The use of e-learning on medical education for mountain rescuers concerning hypothermia. High Alt Med Biol 2018; 19: 272-9. doi: 10.1089/ham.2018.0050 https://doi.org/10.1089/ham.2018.0050 PMid:30010429 PMCid:PMC6157343 |
||||
| 22.Buono FD, Marks A, Lee D. Virtual reality in medical education. Cyberpsychol Behav Soc Netw 2024; 27: 361-2. doi: 10.1089/cyber.2024.27599.geditorial. https://doi.org/10.1089/cyber.2024.27599.geditorial PMid:38841871 |
||||
| 23. Mumber AA. Corporate standards of teaching medical personnel in the Group of companies Center of Corporate Medicine. Proceedings of the V International Conference on Remote Healthcare. 4-5 September, 2025. Tomsk city. Available at: URL: https://remotehealthcare.ru | ||||
| 24. Paal P, Ellerton J, Summan G, Demetz F, Mair P, Brugger H. Basic life support ventilation in mountain rescue. Official recommendations of the International commission for mountain emergency medicine. High Med Biol 2007; 8: 147-54. https://doi.org/10.1089/ham.2007.1025 PMid:17584009 |
||||
| 25.Grissom CK, Thomas F, James B. Medical helicopters in wilderness search and rescue operations. Air Med J 2006; 25: 18-25. doi: 10.1016/j.amj.2005.10.002 https://doi.org/10.1016/j.amj.2005.10.002 PMid:16413423 |
||||
| 26.Tomazin I, Vegnuti M, Ellerton J, Reisten O, Sumann G, Kersnik J. et al. Factors impacting on the activation and approach times of helicopter emergency medical services in four Alpine countries. Scand J Trauma Resusc Emerg Med 2012; 20: 56. doi: 10.1186/1757-7241-20-56 https://doi.org/10.1186/1757-7241-20-56 PMid:22905968 PMCid:PMC3503609 |
||||
| 27. Panchal AR, Bartos JA, Cabanas JG, Donnino MW, Drenna IR, Hirsch KG, et al. Adult Basic and advanced life support: 2020 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2020; 142 (16 Suppl 2); S366-48. https://doi.org/10.1161/CIR.0000000000000918 PMCid:PMC11600417 |
||||
| 28.Smyth MA, Van Goor S, Hansen CM, Fijacko N, Nakagawa NK, Raffay V, et al. European resuscitation Council Guidelines 2025: Adult basic life support. Resuscitation 2025; 215; 110771 https://doi.org/10.1016/j.resuscitation.2025.110771 PMid:41117574 |
||||
| 29.Drennan IR, Berg KM, Bottiger BW, Chia YW, Couper K, Crowley C, et al. Advanced Life support: 2025 International Liazon Committee on Resuscitation Consensus on Science with Treatment Recommendations. Resuscitation 2025; 5 Suppl 2; 110806 https://doi.org/10.1016/j.resuscitation.2025.110806 PMid:41117578 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
