Isolated complete right bundle branch block – findings in the interventricular septum with the speckle-tracking echocardiography: a case report
CASE REPORT
Isolated complete right bundle branch block – findings in the interventricular septum with the speckle-tracking echocardiography: a case report
Article Summary
- DOI: 10.24969/hvt.2026.628
- CARDIOVASCULAR DISEASES
- Published: 26/02/2026
- Received: 27/12/2025
- Revised: 02/02/2026
- Accepted: 03/02/2026
- Views: 1004
- Downloads: 838
- Keywords: Complete right bundle branch block, speckle-tracking echocardiography, interventricular septum
Address for Correspondence: Vitaliy Petrov, Danylo Halytsky Lviv National Medical University, Lviv, Ukraine
E-mail: petrov_vitalii@lnmu.edu.ua
ORCID: Vitaliy Petrov - 0000-0002-2205-5403; Andrii Tytusa - 0000-0003-1445-5703
Vitaliy Petrov, Andrii Tytusa
Danylo Halytsky Lviv National Medical University, Lviv, Ukraine
Abstract
Objective: Isolated complete right bundle branch block (CRBBB) is a known ECG finding in apparently healthy adults. However, the etiology of CRBBB is studied poorly and its prognosis still debatable.
We aimed to demonstrate speckle-tracking imaging findings in a patient with CRBBB.
Case presentation: An apparently healthy lady was found to have a CRBBB on an incidental ECG. Routine echocardiography showed normal cardiac anatomy and function. Speckle-tracking echocardiography depicted preserved global strain of the left ventricle with depressed peak systolic strain of septal apical and mid-septal segments. We present a focal myocardial insult in the area corresponding to the anatomy the right bundle of His. Such correlation may explain the CRBBB present in the otherwise healthy patient.
Conclusion: Speckle-tracking echocardiography in complete right bundle branch block may help to identify the etiology of this conduction disturbance and assist in making the prognosis.
Key words: Complete right bundle branch block, speckle-tracking echocardiography, interventricular septum
Introduction
Isolated complete right bundle branch block (CRBBB) is a known ECG finding in apparently healthy adults. Estimated prevalence of CRBBB is around 1% in the general population (1).
Once found, the CRBBB is usually treated as benign. Indeed, some reported that isolated CRBBB did not increase lethality risks (2–5). However, others observed that CRBBB contributed to higher risk of cardiac death (1, 6, 7).
What also remains to be identified is the cause of the CRBBB. Very often, routine echocardiography (echo) investigation does not reveal any abnormalities and physicians consider this finding as “incidental” and leave it without clear explanations. We report a case of a young asymptomatic lady with CRBBB who underwent speckle-tracking echo (STE) and was found to have specific findings in her myocardium. The latter may be a clue to further studies of this subject.
Graphical abstract
Case report
A 45-year-old healthy lady applied to conduct a thorough heart examination because her friend had recently experienced a heart attack.
Her past medical history included hepatitis A at the age of 2 years and varicella at the age of 10 years. She also reported seasonal influenza infections in the past years, but without remarkable courses. She did have COVID-19 respiratory infection during the 2020 pandemic, however her symptoms were not severe.
Written consent from the patient was obtained for all procedures and publication of case report. The study was performed in frame of Helsinki 2024 agreement for human studies
The patient had an electrocardiogram (ECG) investigation performed at the age of 38 years as a part of medical investigation while applying for a job at an educational institution – and claimed it was normal.
The patient’s physical investigation did not reveal heart murmur or any signs of heart failure. Her blood pressure was 120/80 mmHg, heart rate 70 beats/min and respiratory rate 16/min. Her laboratory data included normal complete blood cells count and urinalysis.
During the current examination a 12-lead ECG was performed and a CRBBB was found (Fig. 1).
An echo study was conducted (Vivid T8, GE Medical Systems). Routine echo showed normal cardiac anatomy and function. Regarding the dimensions, they were within the normal values as indexed for the body mass index, while the function was normal as assessed with the biplane scanning, tissue Doppler as well as mitral and tricuspid annular plane systolic excursion. Speckle-tracking echo (STE) depicted preserved global strain of the left ventricle (-18.7%) with depressed peak systolic strain of septal apical (-12%) and mid-septal (-14%) segments (Fig. 2).
The patient was informed about the findings and after discussions she was recommended to undergo annual follow-up.
Discussion
In this report, we present a focal myocardial insult in the area corresponding to the distal segment of the right bundle of His. This finding may explain the CRBBB present in the otherwise healthy patient. Although post-inflammatory scar might be the simplest explanation of the focal myocardial malfunction, past medical history of the patient did not allow us to state it.
It is affirmed that the CRBBB results from the bundle damage. The following injury mechanisms have already been under the detailed study: acute coronary obstruction of the vessels feeding the bundle and post-ischemic necrosis in the corresponding area of the interventricular septum (8), acute inflammation and post-inflammatory fibrosis (9, 10), graft rejection after the heart transplantation (11), surgical sutures or incisions (12,13), necrosis after alcohol ablation (14), blunt trauma (15), infiltration with sarcoid granulomas (16).![]()
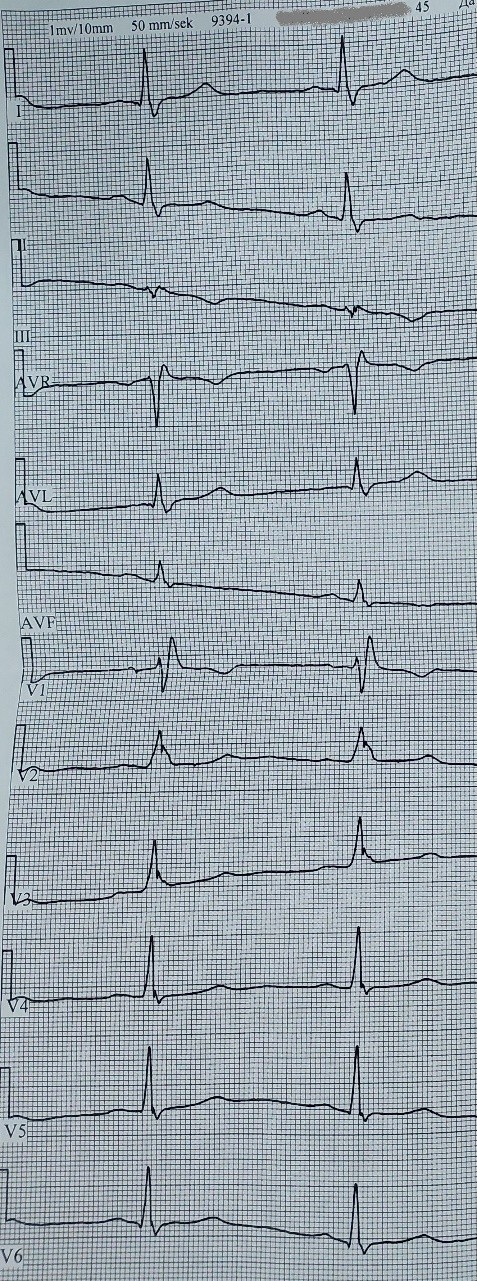
Figure 1. Electrocardiogram depicting the complete right bundle branch block
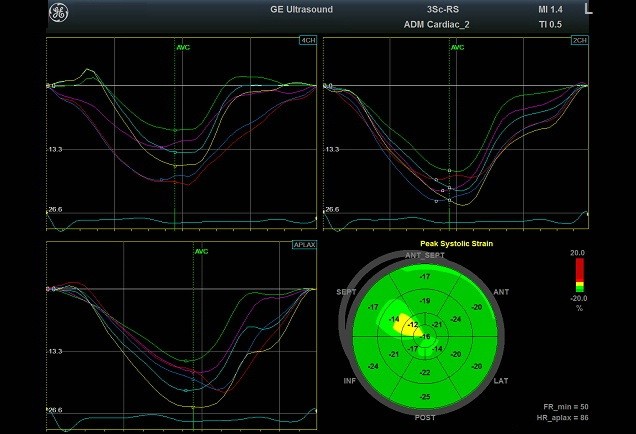
Figure 2. Bull’s eye and tracing patterns of the left ventricle
The right bundle of His may be damaged anywhere along its pathway. Undistinguishable on the ECG, proximal and distal types of the CRBBB have been delineated on highly precise ECG-gated echo (17). In our case, we found depressed peak systolic strain of septal apical and mid-septal segments, corresponding to the distal part of the right bundle, the area where it travels from the interventricular septum to the moderator band (18).
The reasons and topography for the development of CRBBB in individuals without apparently evident cardiac disorders remain to be clarified. We assume that such paucity is due to the underutilization of advanced visualizations technologies, which can identify even minor focal injury patterns. Indeed, the above-mentioned smaller studies used magnetic resonance imaging (MRI) or coronary angiography to identify the region of the myocardial injury in known cardiac disorders (8, 10, 14, 16). However, the larger observations of healthy individuals with CRBBB included ECG or routine echo only (1–7).
The myocardial lesion in our patient was identified with the STE. Recent recommendations of the American Society of Echocardiography suggest using the longitudinal STE as a part of the standard echo examination (19). STE is now a part of the local protocol in our laboratory, which allowed to identify the pattern shown in Figure 2. Therefore, we expect that utilizing STE in large cohorts of healthy adults with CRBBB may help to find explanations of this phenomena and possibly understand why some reported it did not to carry any risks (2–5), while others stated it increased mortality (1, 6, 7). We may carefully suggest that the extent of myocardial involvement as identified on STE could be in the focus of further investigations.
Study limitations
This study has some limitations. The patient refused to conduct MRI in order to confirm the findings. She did not have a comprehensive laboratory panel to identify possible markers of infections. Also, STE of the right ventricle was not performed in this case.
Conclusions
STE demonstrated myocardial lesion in the mid-apical interventricular septum, which corresponded to the distal blockage of the right bundle in an apparently healthy woman. We assume that STE in CRBBB may help to identify the etiology of this conduction disturbance and assist in making the cardiac prognosis of the patient.
Take home message
Speckle-tracking echocardiography may find focal myocardial malfunction if an apparently healthy individual with an isolated complete right bundle branch block.
Topography of myocardial injury as visualized with the speckle-tracking echocardiography corresponds to the conduction system.
Further large-scale investigations of healthy adults with complete right bundle branch block should include longitudinal speckle-tracking echocardiography.
Ethics: Written consent from the patient was obtained for all procedures and publication of case report. The study was performed in frame of Helsinki 2024 agreement for human studies
Peer-review: External and Internal
Conflict of interest: None to declare
Authorship: V.P. and A.T. equally contribute to the management of patients and preparation of case report
Acknowledgements and Funding: None to declare.
Statement on A.I.-assisted technologies use: Author stated they did not use artificial intelligence (A.I.) tools for writing manuscript
Data and material availability: Does not apply
References
| 1. Bussink BE, Holst AG, Jespersen L, Deckers JW, Jensen GB, Prescott E. Right bundle branch block: prevalence, risk factors, and outcome in the general population: results from the Copenhagen City Heart Study. Eur Heart J 2013; 34: 138-46. Doi: 10.1093/EURHEARTJ/EHS291 https://doi.org/10.1093/eurheartj/ehs291 PMid:22947613 |
||||
| 2.Iacovino JR. Mortality analysis of complete right and left bundle branch block in a selected community population. J Insur Med 1997; 29: 91-100. | ||||
| 3.Singer RB. Mortality in insureds with complete right or left bundle branch block. J Insur Med 2007; 39: 8-16. | ||||
| 4.Eriksson P, Wilhelmsen L, Rosengren A. Bundle-branch block in middle-aged men: risk of complications and death over 28 years. The Primary Prevention Study in Göteborg, Sweden. Eur Heart J 2005; 26: 2300-6. Doi: 10.1093/EURHEARTJ/EHI580 https://doi.org/10.1093/eurheartj/ehi580 PMid:16214833 |
||||
| 5. Rankinen J, Haataja P, Lyytikäinen LP, Huhtala H, Lehtimäki T, Kähönen M, et al. Long-term outcome of intraventricular conduction delays in the general population. Ann Noninvasive Electrocardiol 2021; 26: doi: 10.1111/ANEC.12788 https://doi.org/10.1111/anec.12788 PMid:32804416 PMCid:PMC7816813 |
||||
| 6. Casiglia E, Ginocchio G, Marchioro M, Mazza A, di Menza G, Maniati G, et al. Mortality in relation to Minnesota code items in elderly subjects. Sex-related differences in a cardiovascular study in the elderly. Jpn Heart J 1993; 34: 567-77. doi: 10.1536/IHJ.34.567 https://doi.org/10.1536/ihj.34.567 PMid:8301843 |
||||
| 7. Gaba P, Pedrotty D, Desimone C V., Bonikowske AR, Allison TG, Kapa S. Mortality in patients with right bundle-branch block in the absence of cardiovascular disease. J Am Heart Assoc 2020; 9: doi: 10.1161/JAHA.120.017430 https://doi.org/10.1161/JAHA.120.017430 PMid:32924743 PMCid:PMC7792408 |
||||
| 8.Alkindi F, El-Menyar A, Rafie I, Arabi A, Al Suwaidi J, Singh R, et al. Clinical presentations and outcomes in patients presenting with acute cardiac events and right bundle branch block. Angiology 2020; 71: 256-62. Doi: 10.1177/0003319719892159 https://doi.org/10.1177/0003319719892159 PMid:31808355 |
||||
| 9.Freund N, Bremerich J, Buser PT, Zellweger MJ. Cardiovascular flashlight. Transient right bundle branch block in a young patient. Eur Heart J 2009; 30: 1032. Doi: 10.1093/EURHEARTJ/EHP018 https://doi.org/10.1093/eurheartj/ehp018 PMid:19228714 |
||||
| 10. Harimoto K, Kawasaki T, Honda S, Miki S, Kamitani T. Right bundle branch block and ventricular septal fibrosis in patients with hypertrophic cardiomyopathy. J Electrocardiol 2014; 47: 636-41. https://doi.org/10.1016/J.JELECTROCARD.2014.06.010. https://doi.org/10.1016/j.jelectrocard.2014.06.010 PMid:25042853 |
||||
| 11.Kim JH, Oh J, Kim MJ, Kim IC, Uhm JS, Pak HN, et al. Association of Newly Developed Right Bundle Branch Block with Graft Rejection Following Heart Transplantation. Yonsei Med J 2019; 60: 423-8. Doi:10.3349/YMJ.2019.60.5.423 https://doi.org/10.3349/ymj.2019.60.5.423 PMid:31016903 PMCid:PMC6479131 |
||||
| 12.Cui H, Schaff H V., Nishimura RA, Geske JB, Dearani JA, Lahr BD, et al. Conduction abnormalities and long-term mortality following septal myectomy in patients with obstructive hypertrophic cardiomyopathy. J Am Coll Cardiol 2019; 74: 645-55. Doi: 10.1016/j.jacc.2019.05.053 https://doi.org/10.1016/j.jacc.2019.05.053 PMid:31370956 |
||||
| 13. Karadeniz C, Atalay S, Demir F, Tutar E, Ciftci O, Ucar T, et al. Does surgically induced right bundle branch block really effect ventricular function in children after ventricular septal defect closure? Pediatr Cardiol 2015; 36: 481-8. doi: 10.1007/S00246-014-1037-9 https://doi.org/10.1007/s00246-014-1037-9 PMid:25293427 |
||||
| 14. McCann GP, Van Dockum WG, Beek AM, Nijveldt R, Ten Cate FJ, Ten Berg JM, et al. Extent of myocardial infarction and reverse remodeling assessed by cardiac magnetic resonance in patients with and without right bundle branch block following alcohol septal ablation for obstructive hypertrophic cardiomyopathy. Am J Cardiol 2007; 99: 563-7. doi: 10.1016/J.AMJCARD.2006.08.067 https://doi.org/10.1016/j.amjcard.2006.08.067 PMid:17293204 |
||||
| 15. Subramanyam P, Devanabanda AR, Slater WR, Vorsanger M. Transient right bundle branch block: A rare manifestation in cardiac contusion. J Cardiol Cases 2016; 13: 121. doi: 10.1016/J.JCCASE.2015.12.007 https://doi.org/10.1016/j.jccase.2015.12.007 PMid:30546623 PMCid:PMC6280947 |
||||
| 16. Aldweib N, Liu EH, Raina A, Poornima I, Thosani AJ. Rapidly progressive cardiac sarcoidosis: Initial presentation with sinus node dysfunction and right bundle branch block. HeartRhythm Case Rep 2015; 2: 57-9. doi: 10.1016/J.HRCR.2015.09.007 17.Doi Y, Ogawa S, Hiroki T, Arakawa K. Right bundle branch block. Echocardiographic study with special reference to the site of block within the right bundle. Jpn Heart J 1990; 31: 767-76. doi: 10.1536/IHJ.31.767 https://doi.org/10.1536/ihj.31.767 PMid:2084274 |
||||
| 18. Arshad A, Atkinson AJ. A 21st century view of the anatomy of the cardiac conduction system. Trans Res Anat 2022; 28: 100204. doi: 10.1016/J.TRIA.2022.100204 https://doi.org/10.1016/j.tria.2022.100204 |
||||
| 19.Mitchell C, Rahko PS, Blauwet LA, Canaday B, Finstuen JA, Foster MC, et al. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr 2019; 32: 1-64. Doi: 10.1016/J.ECHO.2018.06.004 https://doi.org/10.1016/j.echo.2018.06.004 PMid:30282592 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
