From Editor-in-Chief: On loss of an esteemed genius, our SCIMAGOJr 2025 ranking and SCOPUS citations, current issue, and important scientific documents
EDITORIALS
From Editor-in-Chief: On loss of an esteemed genius, our SCIMAGOJr 2025 ranking and SCOPUS citations, current issue, and important scientific documents
Article Summary
- DOI: 10.24969/hvt.2026.656
- CARDIOVASCULAR DISEASES
- Published: 03/06/2026
- Received: 28/05/2026
- Accepted: 28/05/2026
- Views: 486
- Downloads: 338
- Keywords: Biomedical publishing, guidelines, trials, cardiovascular medicine, surgery, transplantation, internal medicine, public health
Address for Correspondence: Gulmira Kudaiberdieva, Editor-in-Chief, Heart, Vessels and Transplantation
E-mail: editor@hvt-journal.com
ORCID: 0000-0002-4794-8435, 0000-0003-4099-8816
Editorial

From Editor-in-Chief: On loss of an esteemed genius, our SCIMAGOJr 2025 ranking and SCOPUS citations, current issue, and important scientific documents
Graphical abstract
Key words: Biomedical publishing, guidelines, trials, cardiovascular medicine, surgery, transplantation, internal medicine, public health
Dear readers,
I would like to start with sad news (1) on loss a giant in cardiovascular medicine and all ally disciplines, Esteemed Professor Eugene Braunwald. All over the world, for past several decades, cardiologists and cardiac surgeons have become specialists learning how to treat the heart problems from his Textbooks on Heart Diseases, guidelines and articles. The discipline is very complex now, as the new knowledge and new technologies are being emerged constantly. His distinctive ability was to explain these complex matters in simple words to be easily comprehended, the gift of genius people, which reflected in his lectures, textbook and exceptional scientific works frontrunners of evidence-based knowledge and medicine. His legacy will continue contributing to education and training specialists in cardiovascular (CV) medicine and allied disciplines, their growth as scientists as well and we pay a tribute to an esteemed Genius.
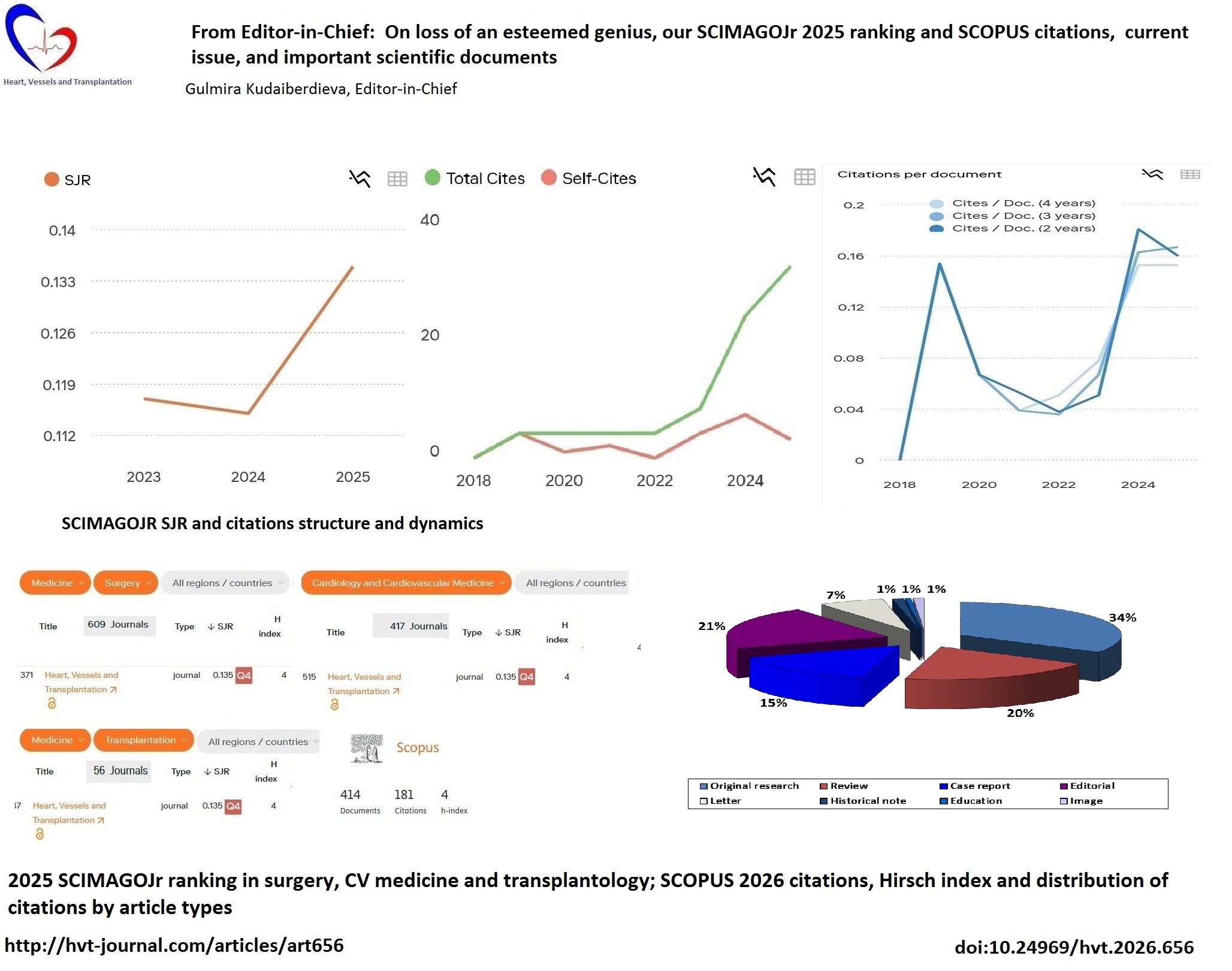
We received our 2025 SCIMAGOJr ranking and SJR – with improvement as compared to 2024 (Fig. 1) (2). SCIMAGOJr SJR is calculated as a number of citations received in 2025 to articles published in previous 4 years - 2021-2024. In 2026, we have increase in SJR to 0.135 from 0.115 in 2025. If we analyze components of SJR formula, we have to look at citations: as can be seen from Figure 1, we see increase in SJR by 17.3% (0.115 in 2024 SJR to 0.135 2025 SJR). We also in parallel see sharp increase in total citations starting from 2022 and further steep climb in 2024, also citations per document sharply increased for past 2 years in 2023 and 2024. Importantly we decreased self-citations rate.
In 2025 – our 2024 SCIMAGOJr rank in surgery was 543 of 579 and CV medicine -381 of 404. In 2026 (Fig. 2) – our 2025 SCIMAGOJr rank in surgery is 515 of 609 journals, thus we climbed up by 28 steps, leaving behind 94 journals (it was 36 in 2025, though number of journals in the list increased by 30, we still have 64 steps in advantage); in CV medicine – our rank is 371 of 417 journals with 47 (was 24 in 2025) journals behind us, we ascended 10 steps up in CV medicine – from 381 to 371, out transplantation ranking is 47th of 56. We are Q4 in all disciplines, and our Hirsch index is 4.
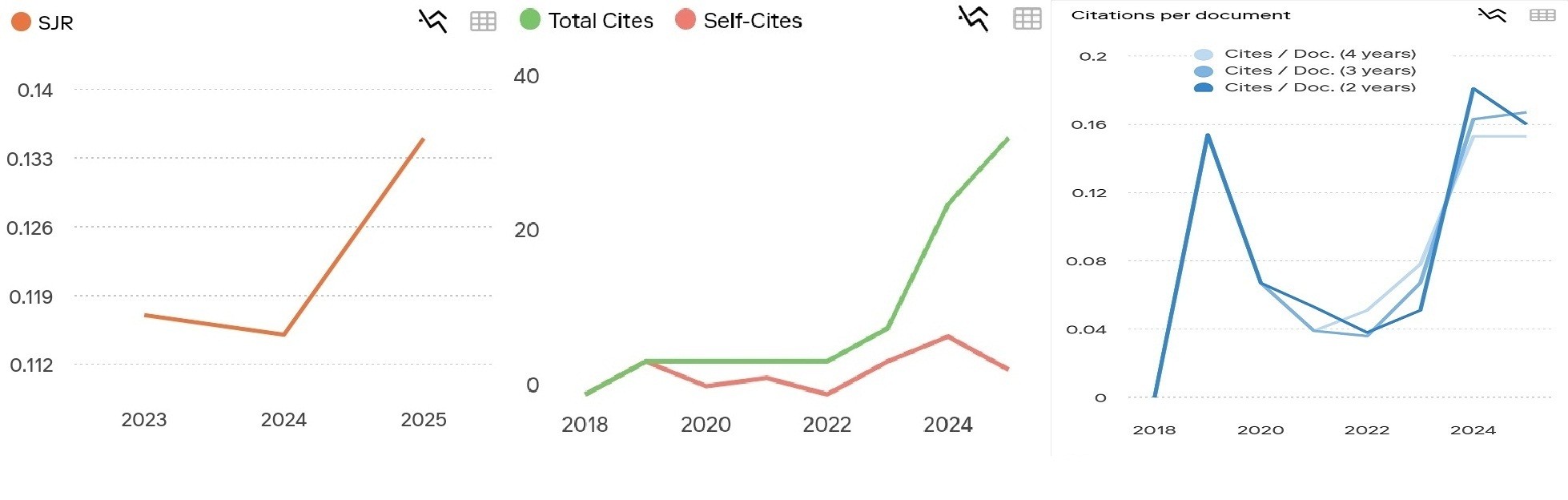
Figure 1. SCIMAGOJR SJR and citations structure and dynamics
We expect SCOPUS 2025 ranking to be released in June 2026, for now I would like to share our current status of citations and CiteScore that are renewed every month in SCOPUS database (3). Our Citescore 2025 is 0.3 as compared to 2024-0.2. If we analyze SCOPUS citations (Fig. 3), we see that number of citations significantly increased to 181 in 2026 and 27.7% of all published articles (115 of 414) have citations, our Hirsch index is 4.
Analysis of cited articles by type, shows that of 115 cited articles 35% are original research, 17% - reviews, 15% - case reports, editorials 20%, letters 8% and historical notes, education and image-5% of articles. We observe that cited review articles (from 13% to 17%) and case reports (from 10 to 15%) are increased since to 2025.
Analysis of citations distribution by the type of articles demonstrates that 34% of 181 citations are earned by original research, 20% - by review articles, 15% - by case reports, 21% by editorials, and 7% by letters, 3% by other historical notes, education and image. Thus as compared to 2025 we have improvement in quality of reviews and case reports, that can be explained that we published in 2 last year’s more systematic reviews, meta-analysis and our case reports deserve attention as describing innovative approaches and rare cases.



Figure 2. 2025 SCIMAGOJr ranking of Heart, Vessels and Transplantation journal on surgery (upper panel), cardiovascular medicine (middle), and transplantation (bottom)
Overall, our progress in SJR (by 17% increase) and increase in citations number, affirm improvement in quality of our articles. We are satisfied by good results and will continue applying our editorial policies, work hard on improvement of content quality, selecting the best evidence, deserving citations and moving to Q3 in a year or two ahead.
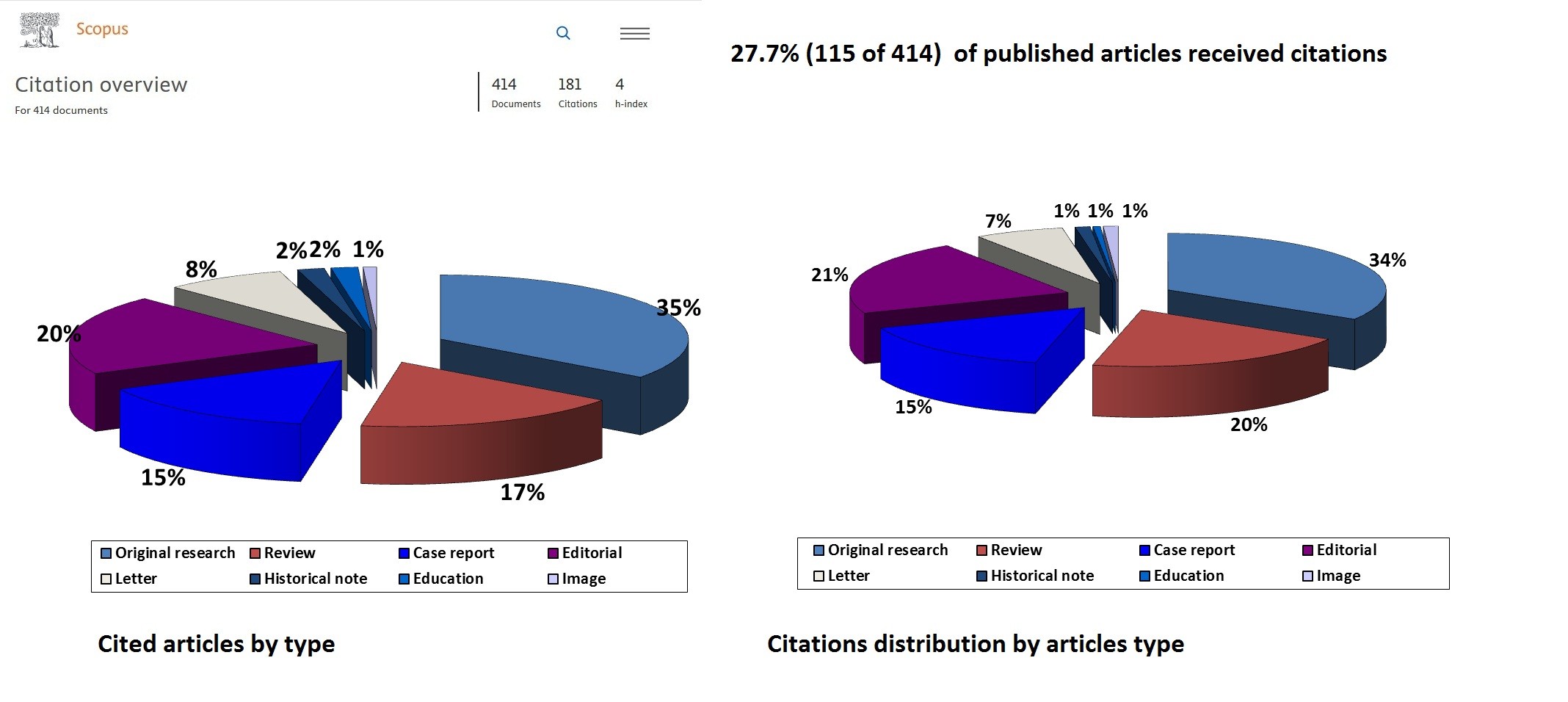
Figure 3. 2026 SCOPUS cited articles and citations distribution by the type of article
In our current June 2026 issue, you can find the Editorials prepared by our editors and invited experts, introducing new guidelines and new evidence-based knowledge important for a wide range of clinical practice physicians: comparison of 2025 ESC/EAS and ACC/AHA guidelines on management of dyslipidemia; comparison of ESC 2024 guidelines and 2025 ACC/AHA guidelines on management of hypertension; and Editorial on advantages of non-thermal pulsed field ablation (PFA) of arrhythmias and its complications that need to be recognized. We brought to your attention several original research studies: of interest for interventional cardiologists and endovascular surgeons –on use of new screw-based access site mechanical compression device aimed to prevent bleeding in transradial percutaneous coronary intervention (PCI); on association of coronary plaque characteristics on computed tomography (CT) angiography with risk factors and stenosis burden; on arterial stiffness features in early peripheral vascular remodeling; on the effect of mutlidisciplinary PERT- pulmonary embolism response team on outcomes of pulmonary embolism; comparison of accuracy of CT venography and color Doppler ultrasonography in the diagnosis of secondary varicose veins; outcomes of endoscopic surgery for cicatricial esophageal narrowing in children; association of growth hormone, insulin-growth factor 1 with growth in children with type 1 diabetes; on public and private institutions partnership in healthcare on example of renal dialysis clinics and their outcomes; and on role of magnesium in exacerbation of chronic obstructive pulmonary disease. You can also find a review - update on management of chronic coronary syndromes; and case reports on rare conditions and complications – ticagrelor hypersensitivity in a patient with acute coronary syndrome who underwent PCI; atrial standstill in a patient with myasthenia gravis treated with conduction system pacing; successful surgical treatment of a ruptured aorto-iliac aneurysm with right arteriovenous fistula; two endovascular surgery applications - innovative endovascular treatment of a patient with secondary Raynaud syndrome and stenting in Sjogren`s syndrome vasculitis. You can read with interest historical note on development of anesthesiology and reanimation in Kyrgyzstan and two patented innovations in CV surgery – surgical technique in reducing septal hypertrophy in hypertrophic cardiomyopathy and implantation technique of aortic conduit for aortic aneurysm to avoid complications.
In 2026, several scientific statements, consensus and position documents, clinical decision pathways and clinical guides have been published by societies: ESC and its associations as EAPCI, EACPR, EHRA, and EACVI; ACC and AHA (4-15). I would like to draw your attention to several important documents that might be of interest for surgeons, CV medicine physicians including imaging, interventions and arrhythmias, vascular surgeons, pediatric surgeons and cardiologists, and interrelated disciplines. Some of them will be prepared by our experts and introduced as Editorials.
At first, I recommend several documents from AHA and ACC for readers treating heart problems in children: pediatricians, pediatric cardiologists and pediatric CV surgeons: on management of acute decompensated heart failure (HF) in children, management of pediatric outpatients with congenital heart disease (CHD) and left-to-right shunts and physical activity in cardiomyopathies in children.
AHA statement on management of acute decompensated HF in children is a concise guide to management of cardiogenic shock (CS) in children. The most frequent acute decompensated HF causes in children are cardiomyopathies and CHDs. Authors offer modified CS stages based on presence of hypotension, use of vasoactive drugs, mechanical circulatory support (MCS, extracorporeal membrane oxygenation (ECMO], Impella, and ventricular assist devices [VAD]). Stage A- no hypotension, no need in vasoactive drugs, no other CS criteria, Stage B – hypotension or vasoactive agents, no other signs of CS, stage C – hypotension and vasoactive drugs plus other criteria for CS, Stage D – MCS plus vasoactive drugs, stage E – circulatory collapse with cardiopulmonary resuscitation. The treatment is based on presence of hypotension or slow output, presence of low perfusion (warm or cold) and congestion (dry and wet) at rest, cardiac and pulmonary failure. In emergency room the following should be performed – assessment of hemodynamic profile, hypotension, low output and congestion signs, evaluation of brain-natriuretic peptide (BNP), chest X-Ray, electrocardiogram (ECG) and echocardiography (echo). Treatment should include loop diuretics if congestion, noninvasive respiratory support and vasoactive agents therapy or both. Indications to intensive care unit (ICU) admission are respiratory failure, unstable cardiac arrhythmias, complex CHDs, use of vasoactive drugs, and use of narcotics for comfort. In ICU monitoring of central venous pressure, near infrared spectroscopy, mixed venous oxygen saturation, blood pressure (BP) and determination of CS stage and MCS need, should be achieved. Treatment includes intermittent or continuous infusion of loop diuretics; endotracheal intubation and ECMO on standby; peripheral, central ECMO, IMPELLA implantation; parenteral nutrition and rehabilitation, wean off vasoactive drugs and start oral HF treatment. All the guidance regarding diagnosis, monitoring and treatment including medicines dosing, respiratory support and MCS implantation and complications, management after acute event are described in details in the document (4).
Clinical guide from ACC (5) on management of outpatients with left-to-right shunt includes following CHDs: atrial septal defect (ASD), atrioventricular septal defect (AVSD), ventricular septal defect (VSD), doubled right ventricle, pulmonary hypertension (PH), Eisenmenger syndrome, and patent ductus arteriosus (PDA). It provides guidance on establishing diagnosis and outpatient evaluation (clinical evaluation, ECG and transthoracic echo [TTE], chest X-Ray and additionally assessment of Qp:Qs ratio, cardiac magnetic resonance imaging [CMR]), complications (presence of vascular disease – cardiac catheterization), risk stratification, treatment and intervention (surgery or transcatheter therapy); frequency of follow-up dependent on age of child and criteria for timing of referral for intervention, as well as management pathways after intervention (clinical evaluation, chest X-Ray, ECG, TTE, endocarditis prophylaxis after surgery and plus transcatheter device specific follow-up and antiplatelet therapy for transcatheter therapy). The management pathways before and after intervention are provided for each CHD (VSD, ASD, partial, transitional and complete AVSD, PDA). General management principles are based on symptoms, right ventricular (RV) or left ventricular (LV) enlargement, right heart or left heart enlargement, presence and severity of atrioventricular or aortic regurgitation, presence of right-to-left shunt, and severity of defect and its repair status. Document is indeed presents the management pathways in clear, succinct and easy to use manner.
Another AHA document I recommend to our readers treating heart problems in children including cardiac surgeons and pediatric cardiologists, pediatricians on physical activity (PA) recommendations in children with cardiomyopathy (CMP) (6). Authors explained advantages of physical activity for children and described recommendations on risk stratification (based on imaging CMR, echo, cardiopulmonary exercise testing, ECG, ECG monitoring, family history and use of risk calculators) and arrhythmia risk assessment of children before recommending PA according to type cardiomyopathy: hypertrophic, restrictive, dilated, arrhythmogenic, dilated due to genetic variants (LMNA, FLNC) and children living with implantable cardioverter-defibrillators.
Competitive and endurance high intensity sports are contraindicated in restrictive CMP and arrhythmogenic CMP with only recreational PA recommendation; recreational PA is also recommended in dilated CMP and hypertrophic CMP, and competitive sport can be recommended if high risk is absent in latter 2 types of CMP. Shared decision-making is recommended for high risk hypertrophic obstructive and restrictive CMPs. Shared decision-making is based on principles: seek, help, assess, reach, and evaluate.
A scientific document from AHA (7) introduces RV dysfunction as adaptive and maladaptive remodeling based on molecular metabolic and imaging detection, including catheter-based diagnosis of RV –pulmonary artery uncoupling Ees/Ea ratio, echo based tricuspid annular plane systolic excursion, RV free wall strain to pulmonary artery systolic pressure, CMR indices of remodeling, cardiac positron emission tomography, and metabolic, inflammatory markers, fibrosis detection defining targets for therapy.
For maternal care ACC published the document (8) on risk assessment for CV diseases in women in postpartum, combining obstetrics/gynecology care and CV risk assessment, screening and treatment: prior to hospital discharge, early late postpartum, and longitudinal care. Authors presented modified WHO risk score and CAPREQ score on risk of maternal CV morbidity and mortality (that can be up to 50% in stage 4) based on presence of ventricular dysfunction, pulmonary hypertension, arrhythmias, CMP, valvular heart disease, aorthopathy, coronary artery disease and other conditions. Authors introduced CV and headache red flags based on symptoms, describe risks leading to arrhythmia, HF and venous thromboembolism in postpartum and provided recommendations regarding monitoring and prevention of hypertensive disorders and screening of CV diseases (8).
In addition, a clinical consensus statement from ESC and ACC on CV abnormalities in masters athletes might be of interest, as you can encounter in your clinical practice athletes with CV complaints, usually ≥35 years old and training 300 minutes per week. Diagnosis and management of atrial fibrillation (AF), ventricular arrhythmias, bradyarrhythmias, coronary atherosclerosis, aortic dilatation, myocardial fibrosis and exercise-induced arrhythmogenic cardiomyopathy are discussed in details in a document (9).
ESC associations published several documents addressing wide audience. One is of interest for interventional cardiologists on intracoronary imaging for optimization of left main coronary artery PCI (10). Authors describe the use of imaging for PCI pre-planning including plaque landing zone, plaque morphology, stent length, stent diameter, stent technique and stent optimization. They explained characteristics IVUS and optical coherence tomography provide: including large-vessel imaging, plague burden, calcium severity, ostial disease, stent size, stent expansion and complications as stent malapposition, stent edge dissection, stent deformation, and tissue protrusion; and situations when physiological assessment is needed (fractional flow reserve, instantaneous wave-free ratio). The guiding role of intracoronary imaging during PCI for left main coronary artery disease is described (10).
Heart failure association of ESC presented a document on management of recent onset CMP, defined as newly detected structural and functional cardiac abnormalities - most often LV dilation and ejection fraction (EF) reduction- detected with 6 months in absence of coronary, valvular, hypertensive and congenital causes. The management and therapy are based on LV reverse remodeling (LVRR). Diagnostic workup includes imaging (ECG, TTE, CMR), biomarker, and genetic testing. Treatment is based on trigger elimination, guidelines directed medical therapy and intervention (cardiac implantable electronic devices [CIEDs], transcatheter edge-to-edge repair [TEER], and ablation if arrhythmia). If there are signs favoring LVRR and recovered EF then therapy withdrawal could be considered, if no and EF only improved, reduced or there is a remission then therapy continues (11). This document deserves studying and principles applied in clinical practice.
For endovascular surgeons and interventional cardiologists, ACC document on requirements and performance measures for transcatheter tricuspid valve implantation (TTVI) would be on interest, including requirements for team (imaging, interventional cardiologist, surgeon), their qualifications, procedural and outcome measures (12). In this context document from ESC EAPCI on preclinical evaluation of novel transcatheter aortic valves would be of importance. Document introduces new valve technologies, their imaging, implantation and performance on preclinical stage (13).
Two documents were introduced during EHRA 2026 congress in April 2026. One is in collaboration with EACVI – on use of intracardiac echocardiography (ICE) for guiding electrophysiological procedures (14). ICE provides opportunity to visualize complex anatomy of atrias in details. Authors described the ICE technical and functional specifications, probes, features rotational, phased –array, 3D-4D and intracardiac catheters available.
The techniques of visualization and mapping of atria and vessels, guiding transseptal puncture and visualization of cavotricuspid isthmus, RV, LV and valves and valvular structures, supported by video materials are described (14).
A scientific statement from EHRA, HRS, APHRS, LAHRS and CHRS on non-thermal PFA for AF has been introduced during EHRA 2026 congress. It provides the physics of pulsed field ablation, its different effects on tissue level as compared to radiofrequency ablation (RFA) or cryoablation and the indications and procedural details for PFA of de novo AF and other arrhythmias. The document describes systems in conjunction of PFA with RFA, and types of catheters used for ablation, technical requirements, anesthesia and procedural details, and complications. Currently the task force writing committee recommends PFA as fist line technology for de novo AF pulmonary vein isolation (15).
Gulmira Kudaiberdieva
Editor-in-Chief
Heart, Vessels and Transplantation
Peer-review: Internal
Conflict of interest: None to declare
Authorship: G.K.
Acknowledgements and funding: None to declare
Statement on A.I.-assisted technologies use: We declare that we did not use AI-assisted technologies in preparation of this manuscript
Data and material availability: Does not apply
References
| 1. Green A. Eugene Braunwald. Lancet 2026; S0140-6736(26)00977-3 doi: 10.1016/ S0140-6736(26)00977-3 | ||||
| 2.SCIMAGOJR. Journal rankings, Available at: URL: www.scimagojr.com | ||||
| 3. SCOPUS sources. Available at: URL: www.scopus.com/sources | ||||
| 4. Cabrera AG, Price JF, Hong BJ, Jeewa A, Tabulov C, Wong SS, et al.Evaluation and Management of the Child With Acute Decompensated Heart Failure: A Scientific Statement From the American Heart Association. Circulation 2026; 153: e1323-e1335. DOI: 10.1161/CIR.0000000000001428 https://doi.org/10.1161/CIR.0000000000001428 PMid:41937629 |
||||
| 5.Sachdeva R, Parthiban A, Birnbaum B, Hancock HS, Jayaram NM, Plummer ST, et al. Outpatient management of isolated left-to-right shunt lesions in pediatric patients: 2026 ACC concise clinical guidance. J Am Coll Cardiol 2026; doi: 10.1016/j.jacc.2025.11.020 https://doi.org/10.1016/j.jacc.2025.11.020 PMid:41885674 |
||||
| 6.Edelson JB, Baker-Smith CM, Cifra B, Cousino M, Day SM, Drezner JA, et al. Physical Activity in Pediatric Cardiomyopathies: Moving for Health: A Scientific Statement From the American Heart Association. Circulation 2026; 153: e1344-e1358. DOI: 10.1161/CIR.0000000000001431 https://doi.org/10.1161/CIR.0000000000001431 PMid:42021760 |
||||
| 7.Pullamsetti SS, Vanderpool RR, de Man F, de Jesus Perez VA, Hemnes, Mukherjee M, et al; on behalf of the Council on Cardiopulmonary, Critical Care, Perioperative, and Resuscitation; Council on Clinical Cardiology; and Council on Cardiovascular Surgery and Anesthesia. Advanced Molecular, Metabolic, and Imaging Approaches to Characterizing Right Ventricular Failure: A Scientific Statement From the American Heart Association. Circulation 2026;153:e1304-e1322. DOI: 10.1161/CIR.0000000000001422 https://doi.org/10.1161/CIR.0000000000001422 PMid:41924886 |
||||
| 8.Lindley KJ, Bello NA, Berlacher KL, Hameed AB, Lane AD, Mahmoud Z, et al Optimization of postpartum care for patients with and at risk for premature and long-term cardiovascular disease: 2026 ACC expert consensus decision pathway. J Am Coll Cardiol 2026; Doi: 10.1016/j.jacc.2025.11.001 https://doi.org/10.1016/j.jacc.2025.11.001 |
||||
| 9.Thijs M.H. Eijsvogels, Jonathan H. Kim, Vincent L. Aengevaeren, Flavio D'Ascenzi, Tim W. Churchill, Elizabeth H. Dineen, et al. Masters Athletes With Abnormal Cardiovascular Findings A Clinical Consensus Statement of the European Association of Preventive Cardiology of the ESC and the American College of Cardiology. J Am Coll Cardiol 2026; doi: 10.1016/j.jacc.2026.03.025 https://doi.org/10.1016/j.jacc.2026.03.025 PMid:41941267 PMCid:PMC13185526 |
||||
| 10. Thomas W. Johnson, Nieves Gonzal , Jose M. de la Torre Hernandez, Nicolas Amabile , Peter O'Kane, Mirvat Alasnag, et al. Interventional cardiology Intracoronary imaging for left main percutaneous coronary intervention: a clinical consensus statement of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC and the European Bifurcation Club (EBC). Eur Heart J 2026; 00: 1-19. Doi: 10.1093/eurheartj/ehag353 https://doi.org/10.1093/eurheartj/ehag353 PMid:42135060 |
||||
| 11. Skouri H, Abdin A, Mullens W, Bucciarelli Ducci C, Starling RC, der Meer PV, et al. Evaluation and management of recent onset cardiomyopathy in the current era of heart failure therapeutics: a clinical consensus statement of the Heart Failure Association of the ESC. ESC Heart Failure 2026; 13: xvag115. Doi: 10.1093/eschf/xvag115 https://doi.org/10.1093/eschf/xvag115 PMid:42048562 PMCid:PMC13202462 |
||||
| 12 O'Gara PT, Little SH, Badhwar V, Bhave NM, Guibone K, Kapadia SR, et al . Operator and institutional recommendations and requirements for tricuspid interventions: 2026 ACC/AHA/ASE/HRS/STS expert consensus systems of care document. J Am Coll Cardiol 2026; Doi: 10.1016/j.jacc.2026.02.5069 https://doi.org/10.1016/j.jacc.2026.02.5069 |
||||
| 13.Piotr P. Buszman, Juan F. Granada, Nicolas Amabile, Emanuele Barbato, Marco Barbanti, Andreas Baumbach, et al. Comprehensive and Contemporary Pre-clinical Evaluation of Novel Transcatheter Aortic Valves. A Scientific Statement of the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the ESC, the ESC Working Group on Cardiovascular Surgery. Eur Heart J Valv Struct Heart Dis 2026; doi: 10.1093/ehjvshd/xwag039/8676192 https://doi.org/10.1093/ehjvshd/xwag039 |
||||
| 14. Peichl P, Tzeis S, Skowronska M, Asvestas D, Baran J, Michela et al. Intracardiac echocardiography during invasive electrophysiological procedures. A scientific statement of the European Heart Rhythm Association of the ESC, and the European Association of Percutaneous Cardiovascular Interventions of the ESC. Europace 2026; doi: 10.1093/europace/euag059/8651483 https://doi.org/10.1093/europace/euag059 PMid:41973950 |
||||
| 15. Kühne M, Badertscher P, Andrade JG, Anic A, Chun J, Russo AD, et al. Pulsed field ablation for the interventional treatment of atrial fibrillation. A Scientific Statement of the European Heart Rhythm Association (EHRA) of the ESC, the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS) and the Canadian Heart Rhythm Society (CHRS). Europace 2026; doi: 10.1093/europace/euag080/8651392 https://doi.org/10.1093/europace/euag080 PMid:41968953 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
