Improved perfusion following arterial stenting in peripheral vasculitis secondary to Sjögren’s syndrome: A case report
CASE REPORT
Improved perfusion following arterial stenting in peripheral vasculitis secondary to Sjögren’s syndrome: A case report
Article Summary
- DOI: 10.24969/hvt.2026.657
- CARDIOVASCULAR DISEASES
- Published: 03/06/2026
- Received: 28/04/2026
- Revised: 26/05/2026
- Accepted: 26/05/2026
- Views: 438
- Downloads: 322
- Keywords: Sjögren syndrome, vasculitis, stents, autoimmune diseases, case report
Address for Correspondence: Mada Ilham Bawono, Dadi Keluarga General Hospital, Purwokerto, Indonesia
Email: Madailham.mi@gmail.com
ORCID: Mada Ilham Bawono - 0009-0008-4938-8030
Improved perfusion following arterial stenting in peripheral vasculitis secondary to Sjögren’s syndrome: A case report
Mada Ilham Bawono1,2*, Arif Prasetyo Utomo3
1General Practitioner, Dadi Keluarga Purwokerto General Hospital, Purwokerto, Indonesia
2Faculty of Medicine, Jenderal Soedirman University, Purwokerto, Indonesia
3Department of Cardiothoracic and Vascular Surgery, Moewardi General Hospital, Surakarta, Indonesia
Abstract
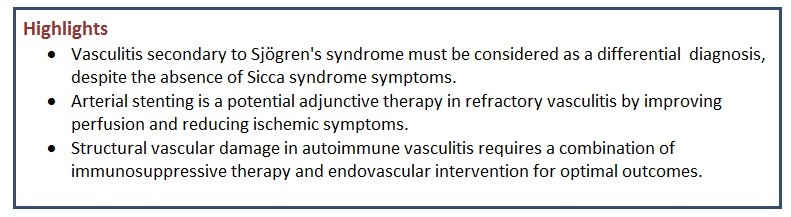
Objective: To report a rare case of peripheral vasculitis secondary to Sjögren's syndrome and to evaluate the outcome of arterial stenting.
Case Presentation: A 42-year-old Javanese male complained of pain on his left toe, worsened by activity. Physical examination revealed an amputation scar on the third toe, pallor and coolness of the left foot, decreased dorsalis pedis and popliteal pulses, and undetectable oxygen saturation. Digital subtraction angiography and multislice computed tomography angiography suggested vasculitis. Immunological evaluation showed antinuclear antibody (ANA) positivity (1:100, nuclear and cytoplasmic fine speckled pattern) and positive Ro-60. Other autoantibodies (La/SS-B, Ro-52, dsDNA, Sm) were negative. This evaluation indicated vasculitis secondary to Sjögren's syndrome. The treatment of this patient included immunosuppressive therapy and arterial stenting, which resulted in improved blood flow.
Conclusion: Despite its limitations, this case report provides valuable insights such as autoimmune etiology should be considered as a differential diagnosis in cases of vasculitis, potential of arterial stenting as adjunctive therapy, and importance of interprofessional collaboration.
Key words: Sjögren syndrome, vasculitis, stents, autoimmune diseases, case report
Introduction
Sjögren’s syndrome is an autoimmune disease with a prevalence of 22 to 32 cases per 100,000 individuals (1). Sjögren’s syndrome also significantly reduces quality of life and can lead to serious complications such as blindness, cognitive dysfunction, kidney disorders, and vasculitis (2, 3). Sjögren’s syndrome also presents with subtle and non-specific manifestations, and the clinical manifestations of Sjögren’s syndrome can be divided into two categories, namely glandular manifestations and extraglandular manifestations (4).
Glandular manifestations are clinical features that commonly occur in patients with Sjögren’s syndrome, such as dry eyes and dry mouth, whereas extraglandular manifestations of Sjögren’s syndrome often vary, ranging from myalgia, xeroderma, Raynaud phenomenon, and cognitive dysfunction due to vasculitis and many others (4).
Graphical abstract
The diverse clinical manifestations of Sjögren’s syndrome determine the most appropriate therapy challenge; currently, the main therapy for Sjögren’s syndrome is the administration of eye drops to manage glandular manifestations and the use of immunosuppressants for extraglandular manifestations. However, the administration of immunosuppressants for extraglandular manifestations is often not sufficient (5, 6).
Therefore, this study presents a case of arterial stenting and immunosuppressive therapy in a patient with vasculitis secondary to Sjögren’s syndrome. It is expected that this case report contributes to the existing literature on autoimmune vasculitis and provides insight for the development of individualized therapeutic approaches.
Case report
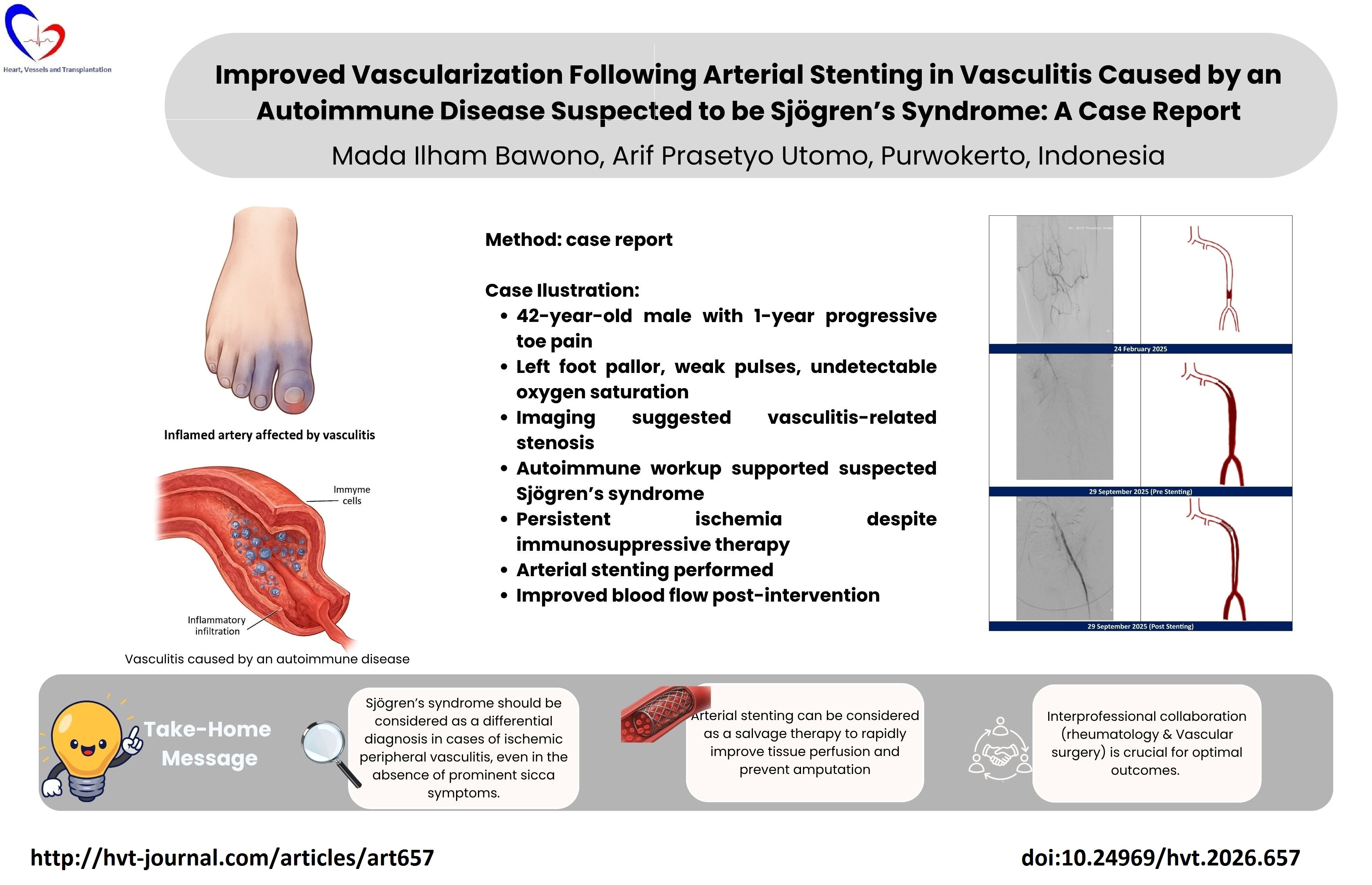
A 42-year-old Javanese male presented to the Thoracic, Cardiac, and Vascular Surgery clinic with a complaint of pain at the tips of his left toes; this complaint had been present and persistent for more than one year, and the pain worsened when the patient walked long distances. The patient denied symptoms such as dry eyes, dry mouth, dry skin, facial redness, or other related complaints. The patient’s past medical history and clinical progression over the past year can be observed in detail in Figure 1. The patient reported a history of epilepsy, with the last seizure occurring two years ago. The patient denied any family history of hereditary or autoimmune diseases.
A comprehensive physical examination was conducted to evaluate autoimmune disorders. Signs such as parotid gland enlargement, oral mucosal atrophy, dental caries, palpable purpura, Raynaud's phenomenon, and signs like arthritis were not found. Upon vascular examination, the patient’s left toes appeared paler compared to the right toes. During palpation, the left foot felt cold, the pulsation of the dorsalis pedis and popliteal arteries of the left foot was decreased, and the capillary refill time of the left foot was >5 seconds. Oxygen saturation in the left toes was undetectable, whereas the right toes showed an oxygen saturation of 98%. Vascular assessment via ankle-brachial index (ABI) revealed a value of 0.6 on the left limb, indicating moderate ischemia.
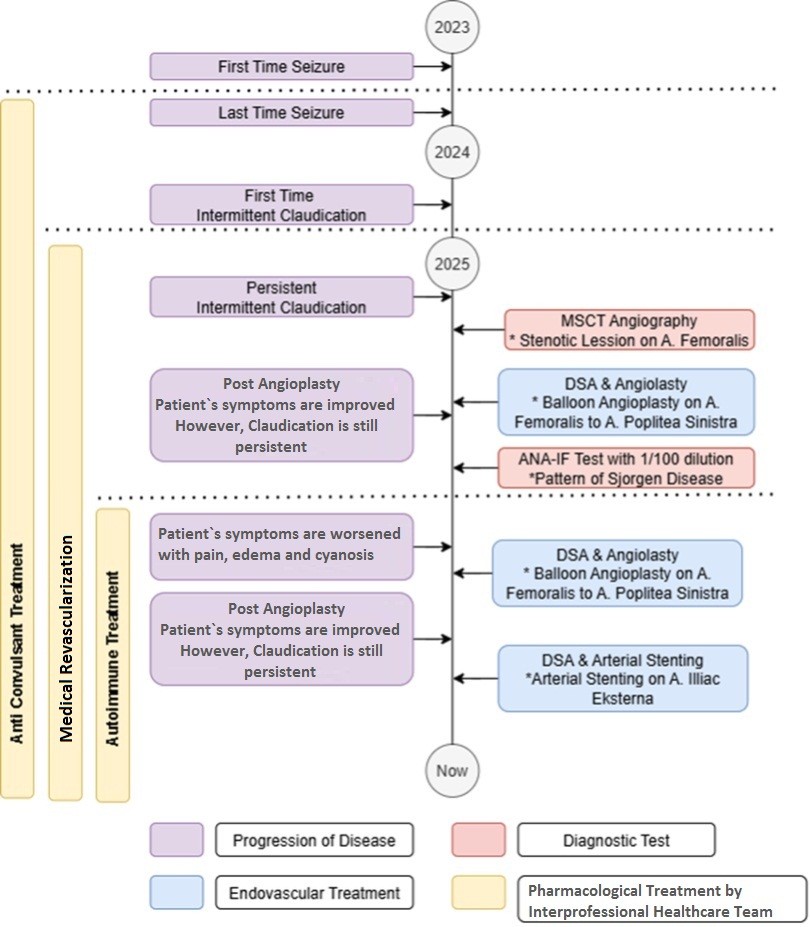
Figure 1. Timeline of the patient’s disease progression
ANA-IF – antinuclear antibodies- immunofluorescence test, DSA – digital subtraction angiography, MSCT – mutlislice computed tomography
Prior multislice computed tomography (MSCT) angiography performed on the lower extremity showed stenosis at the distal one-third of the left superficial femoral artery, total stenosis at the left popliteal artery, and diffuse partial stenosis from the proximal to distal thirds of the left posterior tibial, peroneal, and dorsalis pedis arteries. Blood flow was totally occluded in the left plantar artery.
The patient underwent various diagnostic tests, such as MSCT angiography and digital subtraction angiography; these diagnostic tests showed that the patient experienced stenosis caused by vasculitis. The patient also underwent immunological evaluation that showed antinuclear antibody (ANA) positivity (1:100, nuclear and cytoplasmic fine speckled pattern) and positive Ro-60 (TROVE 2, human RNA-binding protein that regulates misfolded noncoding RNAs). Other autoantibodies (La/SS-B [lupus LA protein-Sjogren syndrome type B protein], Ro-52 [cellular protein and key autoantibody target], dsDNA [double-stranded DNA], Sm [core protein that help process RNA]) were negative, which supported a diagnosis of autoimmune vasculitis secondary to Sjögren’s syndrome, characterized by prominent vascular involvement.
The patient has received various therapies as explained in Figure 1; currently, the patient continues anti-convulsant therapy (phenytoin 3×100 mg, lamotrigine 1×50 mg, gabapentin 1×100 mg, alprazolam 1×0.5 mg), medical revascularization (beraprost 2×20 mcg), and immunosuppressive therapy (Lameson 4-4-0 [methylprednisolone], Myfortic [mycophenolat mofetil] 2×180 mg, Plaquenil [hydroxychloroquine] 1×200 mg). The patient also underwent two endovascular therapies, namely balloon angioplasty to dilate the blood vessels; however, despite all these therapies, the patient’s symptoms persisted and even progressed, leading to arterial stenting on September 29, 2025. The decision to perform endovascular stenting was established through a multidisciplinary approach involving Thoracic, Cardiac, and Vascular Surgery, Interventional Cardiology, and Internal Medicine (Allergy and Immunology). Because the patient had a complex immunological background, the patient required optimization of immunosuppressant therapy (methylprednisolone, mycophenolate mofetil, hydroxychloroquine) managed by the allergy and immunology team. Preprocedural evaluation was performed by the cardiology team who optimized the antithrombotic therapy. The patient initially used an anticoagulant, warfarin, and was replaced with clopidogrel 75 mg daily, cilostazol 100 mg, and beraprost 20 mcg for postprocedural therapy to reduce the risk of stent thrombosis and optimize distal perfusion.
Endovascular intervention was performed via a retrograde approach through the right common femoral artery using a 6 Fr sheath. A cross-over maneuver to the left iliac artery was performed. Angiography examination showed total occlusion of the left external iliac artery up to 12 cm from the bifurcation. This lesion was successfully crossed using a 0.035-inch (260 cm) guidewire. Pre-dilatation was performed with an Oceanus balloon (iVascular, size 4.0 x 150 mm). Subsequently, an iVolution self-expanding stent 6.0 x 80 mm was deployed in the occluded segment. Post-dilatation was performed with a 6.0 x 150 mm Oceanus balloon to optimize stent deployment. Post-dilatation angiogram showed an increase in patient blood flow, although the distal part of the stent still had narrowing (Fig. 2).
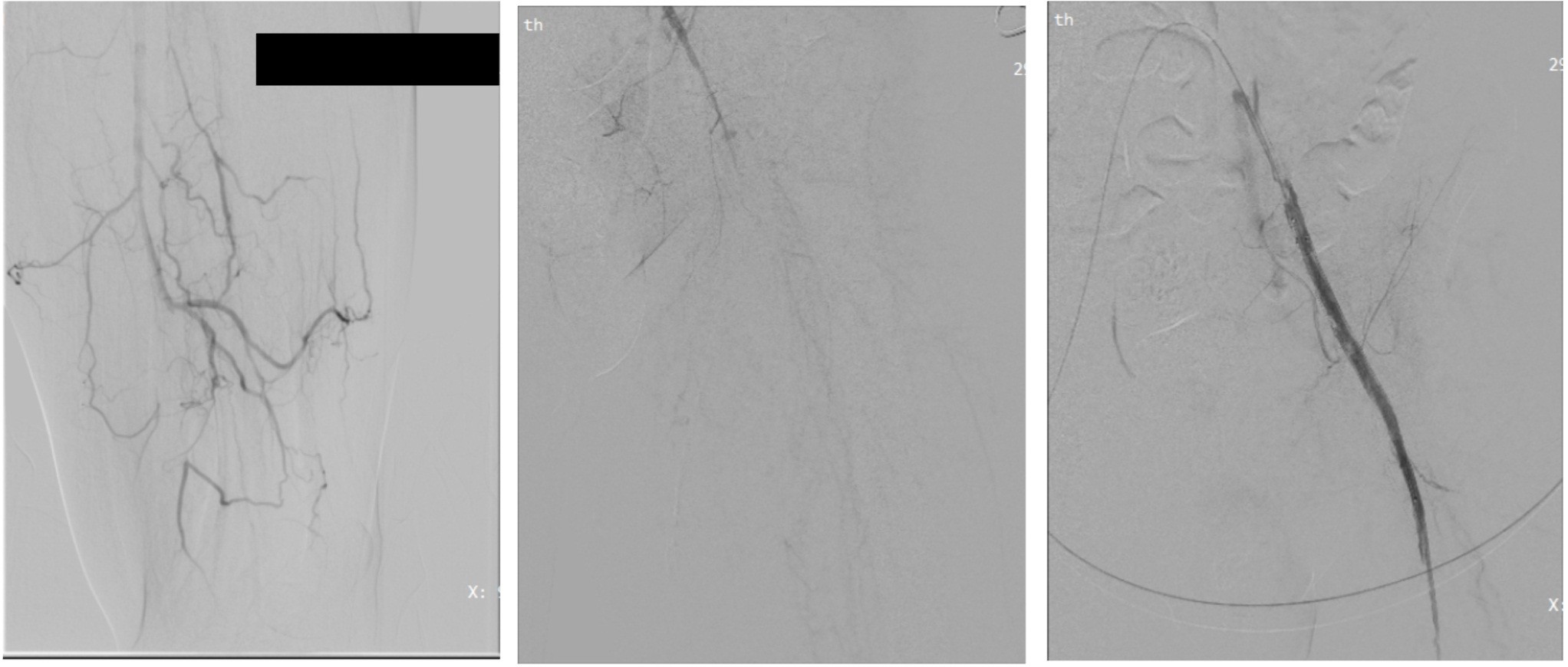
Figure 2. (Left) DSA image dated 24/02/2025, (Center) Pre-stenting DSA image (29/09/2025), (Right) Post-stenting DSA image (29/09/2025)
DSA – digital subtraction angiography
After the patient underwent arterial stenting, the pain in the patient’s foot reduced, although it had not completely resolved. Physical examination revealed the return of warmth to the left foot and a capillary refill time of <2 seconds. Furthermore, distal oxygen saturation improved to 92%. During the 3-day postoperative follow-up, the patient reported pain at the puncture site and experienced mild tingling in the left foot. During the procedure and postoperative observation, no adverse event was observed.
Discussion
This case shows a rare condition of vasculitis caused by Sjögren's syndrome. In primary Sjögren’s syndrome, extraglandular manifestations such as systemic vasculitis occur in approximately 10% of patients and can precede Sicca symptoms in up to 30% of cases (7). The presence of anti-Ro60 antibodies is closely linked to these vasculitic complications (8). In this patient, despite the lack of objective ocular or salivary gland evaluation due to facility constraints, the constellation of high-titer autoantibodies and refractory peripheral ischemia warrants its classification within the primary Sjögren’s syndrome, spectrum, specifically as an isolated, occult extraglandular presentation (9).
This case also shows that a patient with vasculitis secondary to Sjogren syndrome may benefit from arterial stenting. Although not directly related, the literature reports successful stenting in other types of vasculitis, such as Takayasu arteritis and giant cell arteritis (10, 11).
A meta-analysis comparing angioplasty and stenting in Takayasu arteritis found that both have advantages and disadvantages (12).
Pathologically, the primary challenge in autoimmune-induced vasculitis is the presence of active inflammation within the vessel wall, which leads to vascular dysfunction. This inflammation not only causes arterial damage but also increases the risk of long-term restenosis. The clinical correlation of these structural complications is highly relevant in cases of Hughes-Stovin syndrome, Takayasu arteritis, and giant cell arteritis. Although they possess different pathophysiological pathways, these diseases share the common feature of systemic autoimmunity. In these cases, endovascular therapy serves as an adjuvant, and long-term outcomes require the control of the underlying immunological abnormalities (13-15).
In this patient, although immunosuppressive therapy (Lameson, Myfortic, Plaquenil) had been administered to control the systemic immune response, peripheral ischemia remained progressive. This indicates structural damage to the blood vessels (fibrotic stenosis) that is no longer responsive to pharmacological therapy alone. The success of stent placement in this case is likely driven by its ability to provide mechanical support to the arterial wall, which has thickened due to chronic inflammatory infiltrates (16, 17). The use of arterial stenting provides immediate revascularization that is crucial to preserving tissue from further necrosis, especially in patients who already have a history of previous amputation (18). However, it should be noted that long-term success largely depends on control of the underlying autoimmune disease to prevent the development of neointimal hyperplasia within the stent.
Patient perspective
As a police officer, my profession requires high physical mobility, including long-distance walking and rapid tactical movements. This condition significantly hindered my daily duties and professional responsibilities due to debilitating chronic pain. My primary concern was the possibility of progressive limb loss, particularly since I had an amputation of the third digit of my left foot. I feared that, without effective intervention, the necrotic process would extend and result in permanent disability. Despite strict adherence to the prescribed immunosuppressive and pharmacological treatments, my symptoms remained refractory and persistent. Following the arterial stenting procedure, I experienced a notable reduction in pain intensity. Although mild residual sensations remain, I am significantly more comfortable and remain hopeful that this intervention, combined with continued care, will allow me to regain the functional capacity required for my service.
Study Limitations
This case report has several limitations, including that the diagnosis of Sjögren’s syndrome was based on serological markers and clinical manifestations and was not confirmed through salivary gland biopsy or objective Sicca syndrome criteria due to limited available facilities. In addition, the post-stenting follow-up period was very short, only 3 days; therefore, the long-term effectiveness, the risk of stent thrombosis, or restenosis cannot yet be fully evaluated. Finally, as a single case report, the findings cannot be generalized to all patients and require studies with larger populations. This case provides a rare clinical insight into refractory autoimmune vasculitis secondary to Sjögren’s syndrome, showing favorable short-term outcomes after arterial stenting.
Conclusions
In this specific case, the use of arterial stenting demonstrated clinical utility as an adjunctive therapy to improve vascularization in refractory autoimmune vasculitis secondary to Sjögren’s syndrome, especially when immunosuppressive therapy and balloon angioplasty failed to prevent ischemic progression.
Take-home message
Autoimmune vasculitis secondary to Sjögren’s syndrome should be considered as a differential diagnosis in cases of ischemic peripheral vasculitis, even in the absence of prominent Sicca symptoms. In cases of vasculitis that are refractory to immunosuppressive therapy and medical revascularization, arterial stenting can be considered as a salvage therapy to rapidly improve tissue perfusion and prevent amputation. Interprofessional collaboration between vascular surgeons and rheumatologists is essential to ensure that the mechanical success of stenting is complemented by adequate control of systemic inflammation to prevent restenosis.
Ethics: Written informed consent was obtained from the patient for all procedures and for the publication of this case report. This study was conducted in accordance with the principles of the 2024 Declaration of Helsinki for research involving human subjects.
Peer-review: External and Internal
Conflict of interest: None to declare
Authorship: M.I.B. was responsible for patient care coordination, data collection, and drafting the initial manuscript. A.P.U. supervised the study, contributed to the study design and interpretation of data, and critically revised the manuscript for important intellectual content. All authors took equal part in patients management, have read and approved the final version of the manuscript.
Acknowledgments and Funding: None to declare
Statement on A.I Assisted technologies use: The authors used AI-assisted technology through Canva AI solely for generating illustrative images included in the graphical abstract.
No AI-assisted tools were used in the writing, analysis, interpretation, or preparation of the manuscript text.
Data and material availability: Data sharing is not applicable as no datasets were generated or analyzed.
References
| 1. Beydon M, McCoy S, Nguyen Y, Sumida T, Mariette X, Seror R. Epidemiology of Sjögren syndrome. Nat Rev Rheumatol 2024; 20: 158-69. doi: 10.1038/s41584-023-01057-6 https://doi.org/10.1038/s41584-023-01057-6 PMid:38110617 |
||||
| 2. Rojas-Alcayaga G, Herrera A, Espinoza I, Rios-Erazo M, Aguilar J, Leiva L, et al. Illness Experience and quality of life in Sjögren syndrome patients. Int J Environ Res Public Health 2022; 19: 10969. doi:10.3390/ijerph191710969 https://doi.org/10.3390/ijerph191710969 PMid:36078685 PMCid:PMC9518497 |
||||
| 3. Mihai A, Caruntu C, Jurcut C, Blajut FC, Casian M, Opris-Belinski D, et al. The spectrum of extraglandular manifestations in primary Sjögren's syndrome. J Pers Med 2023; 13: 961. doi: 10.3390/jpm13060961 https://doi.org/10.3390/jpm13060961 PMid:37373950 PMCid:PMC10305413 |
||||
| 4. Maleki-Fischbach M, Kastsianok L, Koslow M, Chan ED. Manifestations and management of Sjögren's disease. Arthritis Res Ther 2024; 26: 43. doi: 10.1186/s13075-024-03262-4 https://doi.org/10.1186/s13075-024-03262-4 PMid:38331820 PMCid:PMC10851604 |
||||
| 5. Hellmich B, Sanchez-Alamo B, Schirmer JH, Berti A, Blockmans D, Cid MC, et al. EULAR recommendations for the management of ANCA-associated vasculitis: 2022 update. Ann Rheum Dis 2024; 83: 30-47. doi: 10.1136/ard-2022-223764 https://doi.org/10.1136/ard-2022-223764 PMid:36927642 |
||||
| 6. Carsons S, Blum M. Sjogren syndrome. Treasure island: StatPearls Publishing; 2025. | ||||
| 7. Selmi C, Gershwin ME. Chronic autoimmune epithelitis in Sjögren's syndrome and primary biliary cholangitis: A comprehensive review. Rheumatol Ther 2017; 4: 263-79. doi: 10.1007/s40744-017-0074-2 https://doi.org/10.1007/s40744-017-0074-2 PMid:28791611 PMCid:PMC5696286 |
||||
| 8. Bodakçi E. Clinical characteristics of distinct subgroups of patients with primary Sjögren's syndrome classified by serological profiles: A comparison study. J Pers Med 2024; 14: 967. doi: 10.3390/jpm14090967 https://doi.org/10.3390/jpm14090967 PMid:39338221 PMCid:PMC11433317 |
||||
| 9. Mohanasundaram K, Mani M, Chinnadurai S, Mahendran B, Balaji Ch, Bhoorasamy A, et al. Study on demography and outcome of extraglandular manifestations of primary Sjögren's syndrome. Indian J Rheumatol 2016; 11: 202-6. doi: 10.4103/0973-3698.192690 https://doi.org/10.4103/0973-3698.192690 |
||||
| 10. Konon E, Shahzad A, Quintana Quezada R, Kolfenbach J. Coronary vasculitis in Takayasu's arteriitis: A case report and review of the literature on optimal surgical intervention. J Investig Med High Impact Case Rep 2025;13:23247096251342428 doi: 10.1177/23247096251342427 https://doi.org/10.1177/23247096251342427 PMid:40415671 PMCid:PMC12106977 |
||||
| 11. Dementovych N, Mishra R, Shah QA. Angioplasty and stent placement for complete occlusion of the vertebral artery secondary to giant cell arteritis. J Neurointerv Surg 2012; 4: 110-3. doi:10.1136/jnis.2011.004689 https://doi.org/10.1136/jnis.2011.004689 PMid:21990465 |
||||
| 12. Jeong HS, Jung JH, Song GG, Choi SJ, Hong SJ. Endovascular balloon angioplasty versus stenting in patients with Takayasu arteritis. Medicine 2017; 96: e7558. doi:10.1097/MD.0000000000007558 https://doi.org/10.1097/MD.0000000000007558 PMid:28723782 PMCid:PMC5521922 |
||||
| 13. Trinidad B, Surmachevska N, Lala V. Takayasu arteritis. StatPearls [Internet]; 2023. | ||||
| 14. Ameer M, Vaqar S, Khazaeni B. Giant cell arteritis (Temporal arteritis). StatPearls [Internet]; 2024. | ||||
| 15. Marchetti A, Belvivere L, Argirò R, Kroegler B, Oddi FM, Pennetta F, et al. A rare but fatal Behçet variant: The Hughes-Stovin syndrome-successful case report and new evidence from literature review. Aorta (Stanford) 2023; 11: 156-61. doi:10.1055/s-0043-1777994 https://doi.org/10.1055/s-0043-1777994 PMid:38531384 PMCid:PMC11038734 |
||||
| 16. Che W, Xiong H, Jiang X, Dong H, Zou Y, Yang Y, et al. Stenting for middle aortic syndrome caused by Takayasu arteritis-immediate and long-term outcomes. Cathet Cardiovasc Interv 2018; 91(S1): 623-31. doi: 10.1002/ccd.27492 https://doi.org/10.1002/ccd.27492 PMid:29359504 |
||||
| 17. Khachatryan A, Tamazyan V, Sargsyan M, Haque RU, Cinar T, Alejandro J, et al. Left main snorkel stent thrombosis in association with Takayasu arteritis. Cureus 2024. doi:10.7759/cureus.63761 https://doi.org/10.7759/cureus.63761 |
||||
| 18. Romary DJ, Darling JD, Patel PB, Dash SP, Schermerhorn ML, Lee AM. Systemic immunosuppression does not affect revascularization outcomes in patients with chronic limb-threatening ischemia. J Vasc Surg 2024; 79: 111-9.e2. doi: 10.1016/j.jvs.2023.09.015 https://doi.org/10.1016/j.jvs.2023.09.015 PMid:37717639 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
