ESC/EAS 2025 vs ACC/AHA 2026 dyslipidemia guidelines. From targets to tailoring: a tale of two guidelines
EDITORIALS
ESC/EAS 2025 vs ACC/AHA 2026 dyslipidemia guidelines. From targets to tailoring: a tale of two guidelines
Article Summary
- DOI: 10.24969/hvt.2026.640
- CARDIOVASCULAR DISEASES
- Published: 05/04/2026
- Received: 29/03/2026
- Accepted: 29/03/2026
- Views: 1555
- Downloads: 626
- Keywords: Dyslipidemia, management, guidelines
Address for Correspondence: Fabio Massimo Oddi, Vascular Surgery Unit, Department of Biomedicine and Prevention, University of Rome “Tor Vergata”, Rome, Italy
E-mail: fabio.massimo89@gmail.com
ORCID: Eugenio Martelli – 0000-0001-5764-0082, Fabio Massimo Oddi – 0000-0001- 8081-807X
Assunta Di Vito, Grazia Granata, Manuel Romano, Eugenio Martelli, Fabio Massimo Oddi
Vascular Surgery Unit, Department of Biomedicine and Prevention, University of Rome “Tor Vergata”, Rome, Italy
Key words: Dyslipidemia, management, guidelines
A new update on the management of dyslipidemias has recently been released by the American College of Cardiology and the American Heart Association (ACC/AHA), providing a comprehensive revision of the previous 2018 cholesterol guideline (1). This document should be interpreted alongside the 2025 focused update of the European Society of Cardiology and European Atherosclerosis Society (ESC/EAS) guidelines, which introduced relevant innovations in lipid-lowering strategies and cardiovascular risk assessment (2).
In the last few years, the field of lipid management has undergone major developments, particularly with the introduction of new pharmacological agents and a growing emphasis on individualized cardiovascular risk. In this context, previous work has highlighted the importance of integrating emerging therapeutic strategies with patient-specific risk profiles, reinforcing the need for a more tailored and dynamic approach to dyslipidemia management (3). As a consequence, both European and American societies have updated their recommendations, although with partially different conceptual approaches.
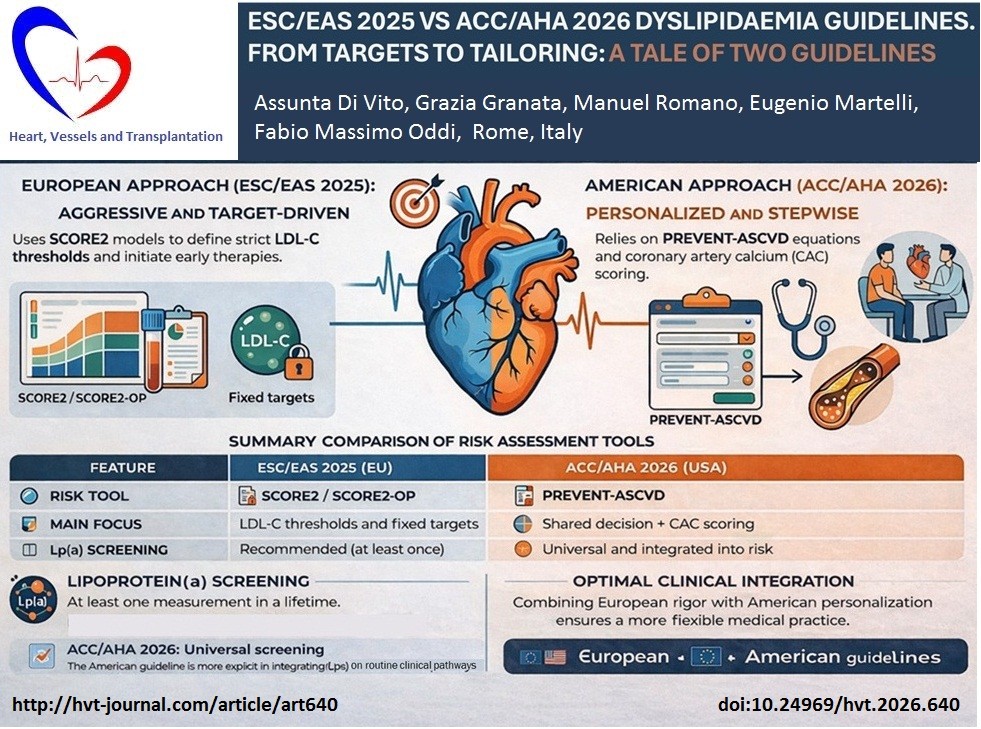
One of the main differences between the two guidelines lies in the general treatment philosophy. The European document maintains a target-driven strategy, emphasizing specific low-density lipoprotein cholesterol (LDL-C) goals according to cardiovascular risk categories. In contrast, the American guideline, while reintroducing LDL-C thresholds, still places significant emphasis on risk estimation and percentage reduction of LDL-C, reflecting a hybrid approach between target-based and intensity-based strategies.
This divergence is particularly evident in cardiovascular risk assessment. The ESC/EAS guideline continues to rely on the SCORE2 and SCORE2-OP systems for risk stratification, maintaining a population-based European model. Conversely, the ACC/AHA guideline introduces the PREVENT ASCVD equations, replacing previous models and expanding risk prediction to both 10- and 30-year horizons.
Graphical abstract
Another important difference concerns the definition of treatment goals. The European guideline strongly reinforces aggressive LDL-C targets, particularly in very high-risk patients, where extremely low levels are recommended. The American guideline, although now incorporating LDL-C goals (e.g., <70 mg/dL or <55 mg/dL in selected populations), still frames treatment primarily in terms of percentage reduction and risk categories, rather than fixed universal targets (Table 1).
|
Table 1. LDL-C targets comparison: The European approach is more aggressive and uniform, while the American guideline applies targets more selectively and contextually. |
||
|
Risk category |
ESC/EAS 2025 |
ACC/AHA 2026 |
|
Very high risk |
<55 mg/dL (optional <40 mg/dL) |
<55 mg/dL (selected patients) |
|
High risk |
<70 mg/dL |
<70 mg/dL |
|
Moderate risk |
Moderate risk <100 mg/dL |
Consider treatment if elevated |
|
Low risk |
Low risk <116 mg/dL |
Lifestyle-based approach |
|
LDL-C – low-density-lipoprotein cholesterol |
||
The role of lipoprotein(a) (Lp(a)) represents an area of convergence but also subtle divergence. Both guidelines recommend at least one lifetime measurement of Lp(a), highlighting its importance as an independent cardiovascular risk factor. However, the American guideline assigns a stronger recommendation for universal screening, integrating it more explicitly into routine risk assessment pathways (3).
Similarly, both documents emphasize the role of apolipoprotein B (apoB), particularly in high-risk patients or those with hypertriglyceridemia. The ACC/AHA guideline explicitly recommends its use to guide therapeutic intensification, while the ESC/EAS document integrates apoB more as an adjunctive marker in selected populations.
A relevant difference emerges in the management of primary prevention. The ESC/EAS guideline adopts a stricter approach, recommending earlier and more intensive lipid-lowering therapy based on absolute risk categories and LDL-C thresholds. On the other hand, the ACC/AHA guideline promotes a more individualized and stepwise strategy, incorporating risk enhancers, coronary artery calcium (CAC) scoring, and shared decision-making to guide treatment initiation (4).
Indeed, the American guideline places a strong emphasis on imaging techniques, particularly CAC scoring, as a tool to refine risk stratification and guide therapeutic decisions. This aspect is less prominent in the European document, which relies more heavily on clinical risk algorithms.
Another major area of divergence concerns the pharmacological approach. The ESC/EAS guideline continues to advocate for a rapid intensification strategy aimed at achieving LDL-C targets as early as possible, often recommending combination therapy upfront in high-risk patients. In contrast, the ACC/AHA guideline generally supports a stepwise intensification, starting with statins and progressively adding ezetimibe, PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitors, or newer agents such as bempedoic acid or inclisiran when needed (Table 2).
|
Table 2. Pharmacological strategies: The ESC/EAS guideline promotes early combination therapy, whereas the ACC/AHA guideline favors a progressive escalation model |
||
|
Step |
ESC/EAS 2025 |
ACC/AHA 2026 |
|
Initial therapy |
High-intensity statin ±combination |
Statin based on risk |
|
Second step |
Early addition of ezetimibe |
Add ezetimibe if needed |
|
Third step |
Early PCSK9 inhibitor in high-risk |
Stepwise PCSK9 inhibitor use |
|
New therapies |
Inclisiran considered |
Inclisiran, bempedoic acid integrated |
|
Overall approach |
Rapid intensification |
Gradual, stepwise escalation |
|
PCSK9 - proprotein convertase subtilisin/kexin type 9 |
||
The American document also provides a more detailed framework for emerging therapies, including inclisiran and novel agents, integrating them into specific clinical scenarios such as severe hypercholesterolemia or statin intolerance.
The management of special populations further highlights differences between the two approaches. The ESC/EAS guideline includes dedicated sections in patients with conditions such as HIV infection or cancer, emphasizing tailored lipid management in these groups. The ACC/AHA guideline expands this concept, providing more granular recommendations across a broader range of populations, including pregnancy, chronic kidney disease, and subclinical atherosclerosis.
Finally, both guidelines underline the importance of lifestyle interventions, although the American document provides a more structured and detailed framework, including explicit recommendations on dietary patterns, referral to dietitians, and long-term behavioral strategies. These recommendations are consistent with previous findings demonstrating that both intensive lipid-lowering strategies and personalized treatment pathways can be effective when appropriately applied in clinical practice (5).
In conclusion, while the ESC/EAS 2025 and ACC/AHA 2026 guidelines share the common goal of reducing atherosclerotic cardiovascular risk through lipid lowering, they differ in several key aspects. The European approach remains strongly target-oriented and aggressive, whereas the American guideline adopts a more personalized, risk-based, and stepwise strategy.
Understanding these differences is crucial for clinicians, as it allows a more flexible and patient-centered application of evidence-based medicine, integrating the strengths of both approaches into every day clinical practice.
Peer-review: Internal
Conflict of interest: None to declare
Authorship: A.D.V., G.G., M.R., E.M., and F.M.O. equally contributed to the preparation of manuscript and fulfilled all authorship criteria
Acknowledgements and funding: None to declare
Statement on A.I.-assisted technologies use: The authors used AI-supported technologies in the preparation of figures .
Data and material availability: Do not apply
References
| 1. Blumenthal RS, Morris PB, Gaudino M, Johnson HM, Anderson TS, Bittner VA, et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of dyslipidemia: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2026; doi: 10.1161/CIR.0000000000001423 https://doi.org/10.1161/CIR.0000000000001423 PMid:41824552 |
||||
| 2. Mach F, Koskinas KC, Roeters van Lennep JE, Tokgözoğlu L, Badimon L, Baigent C, et al; ESC/EAS Scientific Document Group. 2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidemias. Eur Heart J 2025; 46: 4359-78. doi: 10.1093/eurheartj/ehaf190 https://doi.org/10.1093/eurheartj/ehaf190 PMid:40878289 PMCid:PMC12945982 |
||||
| 3. Kronenberg F, Mora S, Stroes ESG, Ference BA, Arsenault BJ, Berglund L, et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Eur Heart J 2022; 43: 3925-46. doi: 10.1093/eurheartj/ehac361 https://doi.org/10.1093/eurheartj/ehac361 PMid:36036785 PMCid:PMC9639807 |
||||
| 4. Mortensen MB, Tybjærg-Hansen A, Nordestgaard BG. Statin eligibility for primary prevention of cardiovascular disease according to 2021 European prevention guidelines compared with other international guidelines. JAMA Cardiol 2022; 7: 836-43. doi: 10.1001/jamacardio.2022.1876 https://doi.org/10.1001/jamacardio.2022.1876 PMid:35793078 PMCid:PMC9260641 |
||||
| 5. Servadei F, Scimeca M, Palumbo V, Oddi FM, Bonfiglio R, Giacobbi E, et al. Aging and sex modify the risk of carotid plaque thrombosis related to dyslipidemic profile. Stroke 2025; 56: 2879-87. doi: 10.1161/STROKEAHA.125.051754 https://doi.org/10.1161/STROKEAHA.125.051754 PMid:40693375 PMCid:PMC12447824 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
