Ticagrelor-induced cutaneous hypersensitivity in a patient with acute coronary syndrome following percutaneous coronary intervention: A case report
CASE REPORT
Ticagrelor-induced cutaneous hypersensitivity in a patient with acute coronary syndrome following percutaneous coronary intervention: A case report
Article Summary
- DOI: 10.24969/hvt.2026.641
- CARDIOVASCULAR DISEASES
- Published: 10/04/2026
- Received: 22/02/2026
- Revised: 30/03/2026
- Accepted: 30/03/2026
- Views: 808
- Downloads: 538
- Keywords: Ticagrelor, acute coronary syndrome, drug-induced rash, hypersensitivity, percutaneous coronary intervention
Address for Correspondence: Raj Sachde, Department of Cardiology, Dr. D. Y. Patil Medical College, Hospital & Research Centre, Dr. D. Y. Patil Vidyapeeth, Pune, Maharashtra, India
Email: rjsachde@gmail.com Mobile: +91 9624092892
ORCID: Ajitkumar Jadhav- 0000-0002-2494-4802; Digvijay Nalawade- 0000-0002-6864-4297; Raj Sachde- 0009-0009-5630-3143; Sridevi Chigulapalli- 0000-0001-5662-5235
Ajitkumar Jadhav, Digvijay Nalawade, Raj Sachde, Sridevi Chigulapalli
Department of Cardiology, Dr. D. Y. Patil Medical College, Hospital & Research Centre, Dr. D. Y. Patil Vidyapeeth, Pune, Maharashtra, India
Abstract
Objective: Ticagrelor is a potent oral P2Y12 receptor inhibitor widely used as part of dual antiplatelet therapy in patients with acute coronary syndrome undergoing percutaneous coronary intervention (PCI). Although generally well tolerated, hypersensitivity reactions to ticagrelor are rarely reported.
Case presentation: We describe a case of a 56-year-old male with acute coronary syndrome who developed generalized pruritus, urticarial rash, and angioedema following initiation of ticagrelor after intravascular ultrasound–guided PCI. Prompt recognition, exclusion of infective causes, and substitution with prasugrel led to complete symptom resolution without ischemic complications.
Conclusion: This case highlights the importance of early identification of ticagrelor-induced cutaneous hypersensitivity and demonstrates the safety of switching to an alternative P2Y12 inhibitor in the post-PCI setting.
Key words: Ticagrelor, acute coronary syndrome, drug-induced rash, hypersensitivity, percutaneous coronary intervention
Introduction
Dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 receptor inhibitor forms the cornerstone of management in patients with acute coronary syndrome (ACS), particularly following percutaneous coronary intervention (PCI) (1). Ticagrelor, a reversible oral P2Y12 inhibitor, has demonstrated superior ischemic outcomes compared with clopidogrel in ACS but is associated with adverse effects such as dyspnea, bradyarrhythmias, and bleeding (2). Cutaneous hypersensitivity reactions to ticagrelor are uncommon and sparsely reported in literature (3, 4). Early recognition is essential, as continued exposure may lead to progression of symptoms, while abrupt cessation without an alternative antiplatelet agent carries a risk of stent thrombosis.
We report a rare case of ticagrelor-induced cutaneous hypersensitivity presenting with urticarial rash and angioedema shortly after PCI.
Graphical abstract
Case report
A 56-year-old male with a known history of hypothyroidism on regular treatment presented with complaints of sudden-onset rest angina for seven days, associated with dyspnea on exertion (New York Heart Association class II). There was no prior history of coronary artery disease, drug allergy, or recent infection. Written informed consent was obtained from the patient for examinations, coronary intervention, the medical management, and the publication of this case report and associated images.
On admission, the patient was hemodynamically stable. Vital parameters were within normal limits. Cardiovascular, respiratory, abdominal, and neurological examinations were unremarkable.
Electrocardiography (ECG) revealed changes suggestive of an evolved inferior wall myocardial infarction. Baseline laboratory investigations, including renal and hepatic function tests, were within normal limits.
Coronary angiography demonstrated critical stenotic lesions in the left anterior descending artery and a major obtuse marginal branch. The patient underwent intravascular ultrasound (IVUS)–guided PCI to both vessels with optimal angiographic and IVUS results. Post-procedure, the patient received a loading dose of ticagrelor and was initiated on standard DAPT with ticagrelor and aspirin. The post-procedural course was uneventful, and the patient was discharged the following day in stable condition.
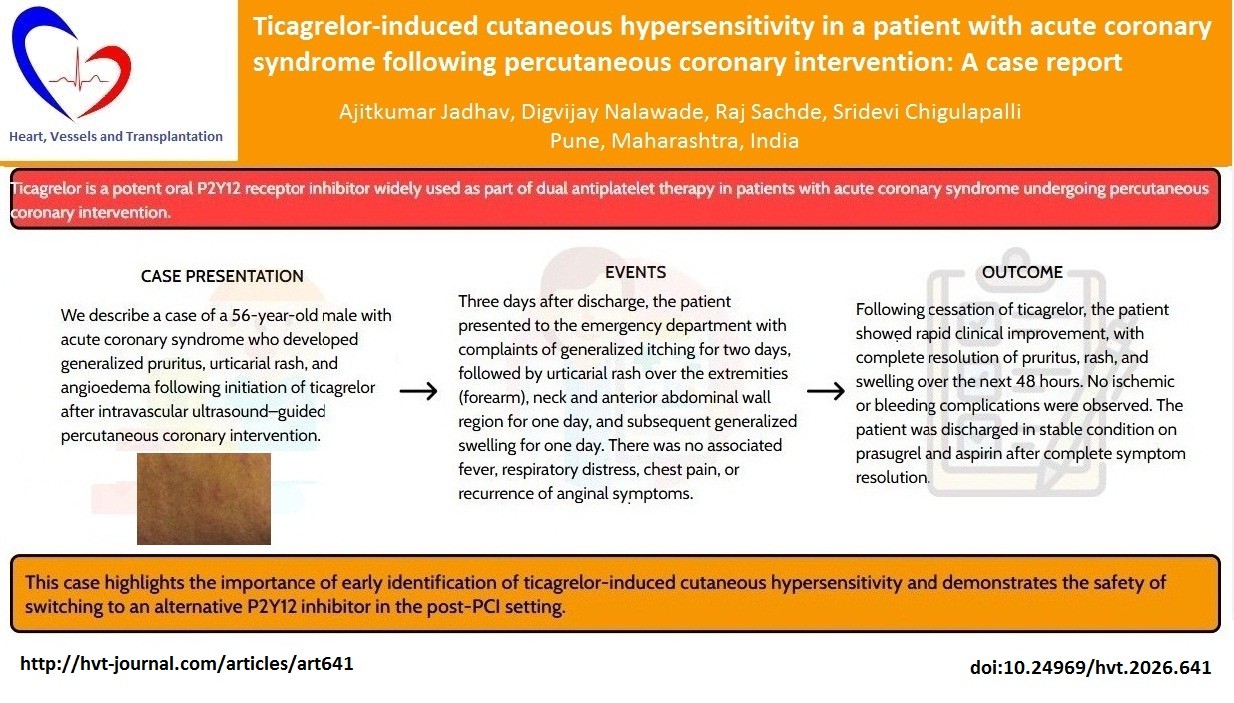
Three days after discharge, the patient presented to the emergency department with complaints of generalized itching for two days, followed by urticarial rash over the extremities (forearm), neck and anterior abdominal wall region for one day (Fig. 1-3), and subsequent generalized swelling for one day. There was no associated fever, respiratory distress, chest pain, or recurrence of anginal symptoms.
On examination, the patient was vitally stable. Dermatological examination revealed urticarial wheals over the limbs and neck with mild generalized edema. There were no mucosal lesions or features suggestive of anaphylaxis. Systemic examination was otherwise unremarkable. Repeat ECG showed no new ischemic changes.
A dermatology consultation was sought. Differential diagnoses included drug-induced hypersensitivity reaction versus infective etiology. Laboratory markers of infection and inflammation, including complete blood count and inflammatory markers were within normal limits. The platelet count remained stable at 210,000/ µL and coagulation tests were within normal limits, ruling out thrombocytopenia or systemic coagulopathy. There were no clinical signs of bleeding.
A multidisciplinary team (MDT) consisting of cardiologists and dermatologists was convened to determine the optimal management strategy.

Figure 1. Cutaneous hypersensitivity reaction affecting the upper limb. (A) Rash over the proximal arm.
(B) Extension of lesions along the forearm after ticagrelor initiation post–percutaneous coronary intervention.
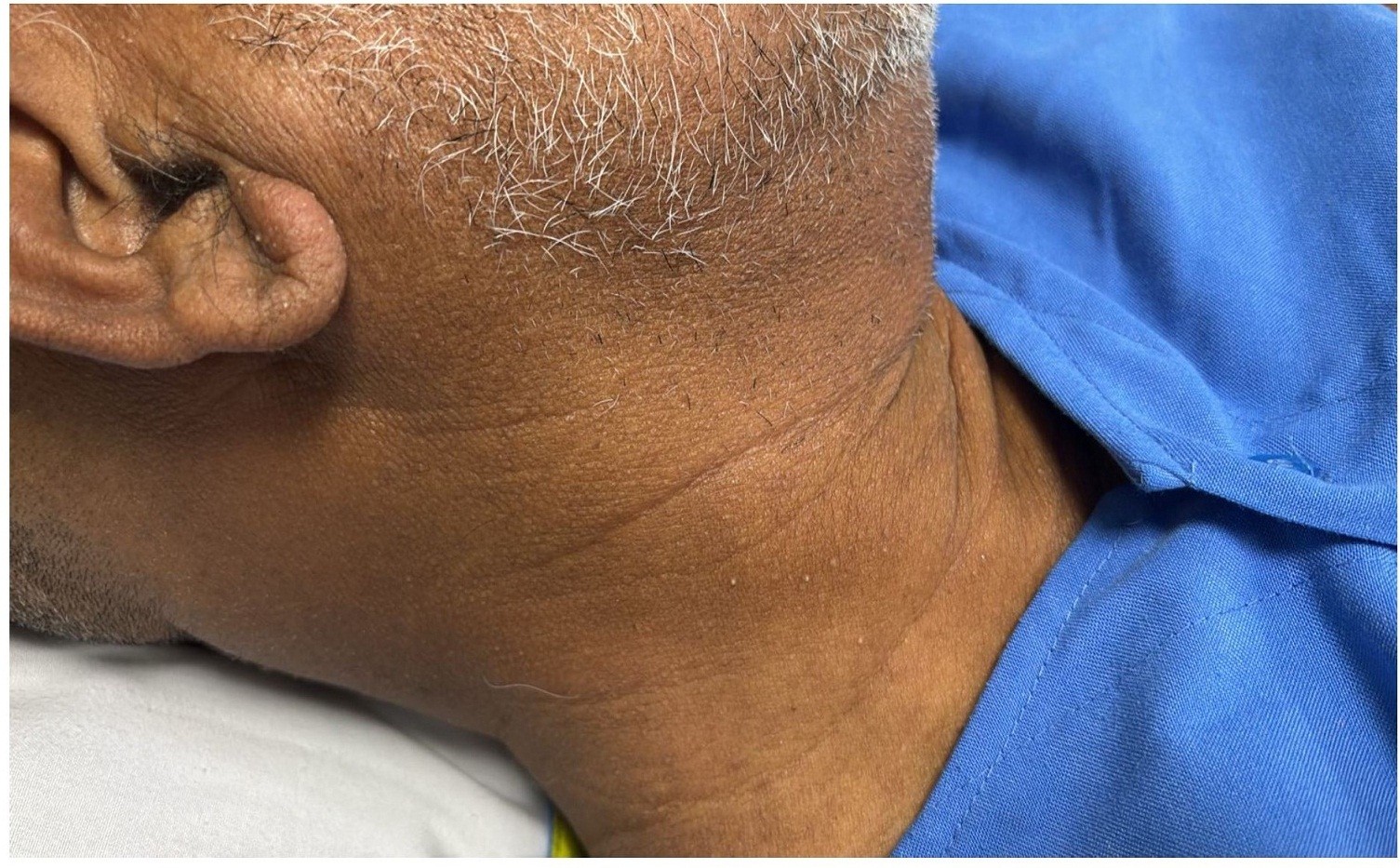
Figure 2. Clinical photograph showing a diffuse erythematous maculopapular rash involving the neck
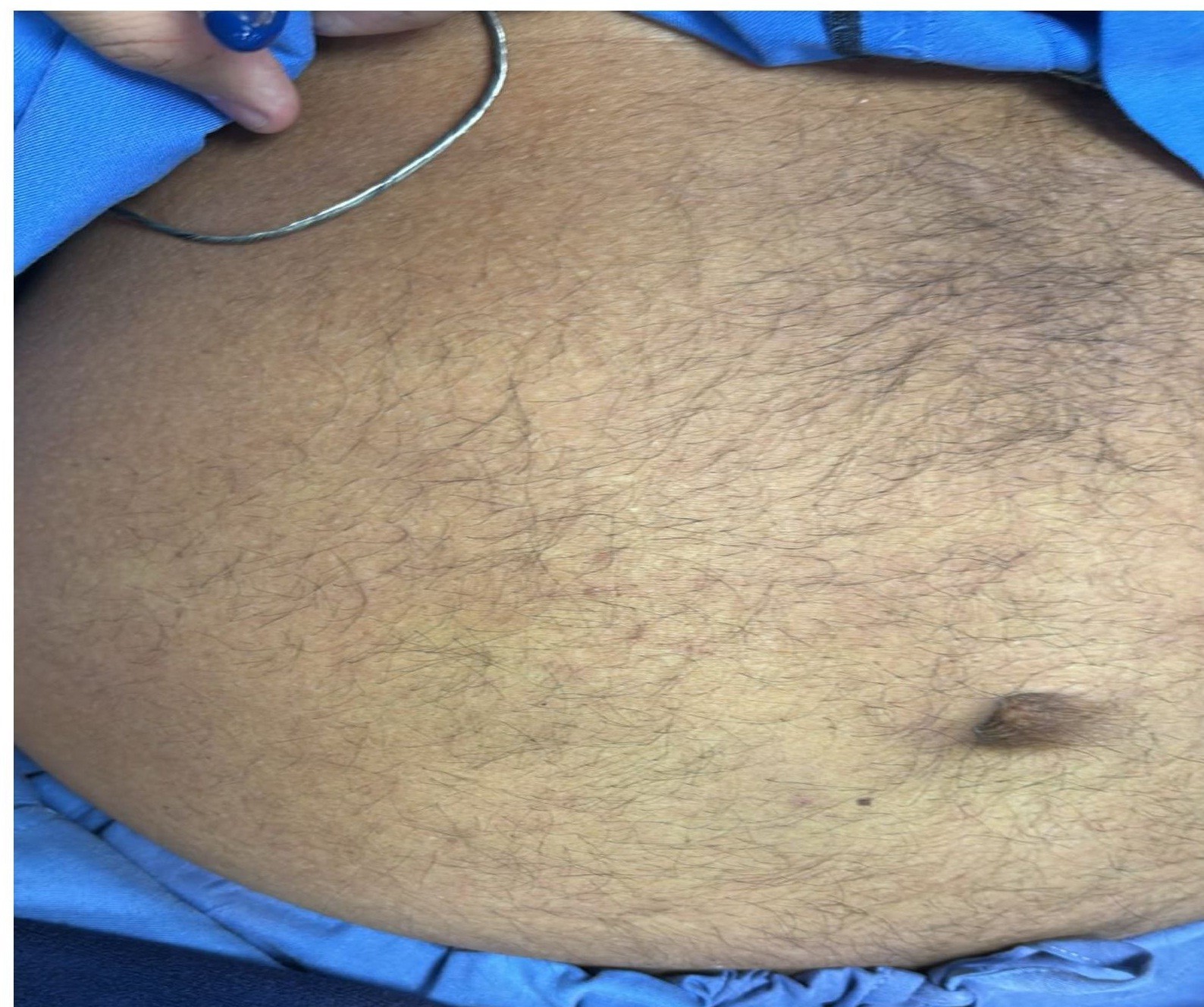
Figure 3. Clinical photograph showing a diffuse erythematous maculopapular rash involving the anterior abdominal wall
The MDT’s primary concern was the high risk of stent thrombosis if P2Y12 inhibition was interrupted, weighed against the risk of the hypersensitivity reaction progressing to anaphylaxis.
The consensus was to switch the patient to an alternative class of P2Y12 inhibitor immediately. Prasugrel was selected due to its potent antiplatelet effect and its distinct chemical structure compared to ticagrelor.
Given the temporal association with ticagrelor initiation and absence of other identifiable causes, ticagrelor-induced hypersensitivity was suspected. Ticagrelor was immediately withheld, and the patient was switched to prasugrel with a loading dose of 60 mg followed by 10 mg once daily, in combination with aspirin.
Following cessation of ticagrelor, the patient showed rapid clinical improvement, with complete resolution of pruritus, rash, and swelling over the next 48 hours. No ischemic or bleeding complications were observed. The patient was discharged in stable condition on prasugrel and aspirin after complete symptom resolution.
Discussion
Ticagrelor is a cyclopentyl-triazolo-pyrimidine that inhibits platelet aggregation via reversible blockade of the P2Y12 receptor. Hypersensitivity reactions associated with ticagrelor are rare and may manifest as pruritus, rash, urticaria, or angioedema (3). The underlying mechanism is not fully understood but is thought to be immunologically mediated.
In the present case, the close temporal relationship between ticagrelor initiation and symptom onset, absence of infective or inflammatory markers, and prompt symptom resolution after drug withdrawal strongly support a diagnosis of ticagrelor-induced cutaneous hypersensitivity.
Management of such cases is challenging due to the need for uninterrupted antiplatelet therapy post-PCI. An MDT approach was utilized to minimize the 'platelet gap' during the drug switch. Prasugrel was strategically chosen over clopidogrel due to its more rapid onset and potent, predictable platelet inhibition, which was essential given the patient’s recent complex PCI (5). Crucially, as a thienopyridine, prasugrel is chemically distinct from the cyclopentyl-triazolo-pyrimidine structure of ticagrelor. This structural divergence was central to the MDT’s rationale, as it significantly reduces the risk of immunological cross-reactivity. The successful transition without recurrence of symptoms validates the choice of a structurally unrelated but pharmacologically potent alternative.
This case underscores the need for clinicians to maintain a high index of suspicion for drug-induced hypersensitivity reactions in patients presenting with new-onset dermatological symptoms after initiation of antiplatelet therapy.
Conclusion
Ticagrelor-induced cutaneous hypersensitivity, though rare, should be considered in patients presenting with rash, pruritus, or angioedema following initiation of therapy. Early recognition, prompt drug discontinuation, and substitution with an alternative P2Y12 inhibitor such as prasugrel can lead to rapid symptom resolution without compromising antiplatelet efficacy. Awareness of this adverse effect is crucial for timely management and prevention of serious complications.
Ethics: Written informed consent was obtained from the patient for examinations, coronary intervention, the medical management, and the publication of this case report and associated images.
Peer-review: External and internal
Conflict of interest: None to declare
Authorship: A.J., D.N., R.S., and S.Ch. equally contributed to the case management, preparation of manuscript and fulfilled all authorship criteria
Acknowledgements and funding: None to declare
Statement on A.I.-assisted technologies use: The authors used AI-supported technologies in the preparation of graphical abstract
Data and material availability: Do not apply
References
| 1.Shpigelman J, Proshkina A, Daly MJ, Cox D. Personalized dual antiplatelet therapy in acute coronary syndromes: striking a balance between bleeding and thrombosis. Curr Cardiol Rep 2023; 25: 693-710. https://doi.org/10.1007/s11886-023-01892-9 PMid:37261665 PMCid:PMC10307718 |
||||
| 2.Wei P, Wang X, Fu Q, Cao B. Progress in the clinical effects and adverse reactions of ticagrelor. Thromb J 2024; 22: 8. https://doi.org/10.1186/s12959-023-00559-3 PMid:38200557 PMCid:PMC10782624 |
||||
| 3.Lunge S, Doshi SR, Sardesai VR. Ticagrelor-induced dermatological hypersensitivity reaction. Cureus 2025; 17: e85484. https://doi.org/10.7759/cureus.85484 PMid:40625494 PMCid:PMC12230203 |
||||
| 4.Akdogan RE, Chen J, Varon A, Muradova E, Fusco J. Generalized drug eruption secondary to ticagrelor: a case report and review of the literature. Cureus 2023; 15: e34800. https://doi.org/10.7759/cureus.34800 |
||||
| 5.Feng WH, Chang YC, Lin YH, Chen HL, Chen CY, Lin TH, et al. P2Y12 inhibitor monotherapy versus conventional dual antiplatelet therapy in patients with acute coronary syndrome after percutaneous coronary intervention: a meta-analysis. Pharmaceuticals 2023; 16: 232. https://doi.org/10.3390/ph16020232 PMid:37259380 PMCid:PMC9958698 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
