Endoscopic bougienage of cicatricial esophageal strictures in children: Experience of the clinic of the National Center for Maternal and Child Health
ORIGINAL RESEARCH ARTICLE
Endoscopic bougienage of cicatricial esophageal strictures in children: Experience of the clinic of the National Center for Maternal and Child Health
Article Summary
- DOI: 10.24969/hvt.2026.651
- CARDIOVASCULAR DISEASES
- Published: 16/05/2026
- Received: 28/02/2026
- Revised: 20/04/2026
- Accepted: 20/04/2026
- Views: 529
- Downloads: 292
- Keywords: Endoscopy, cicatricial stricture, bougienage, esophageal burns, children
Address for Correspondence: Tatyana A. Akmentyeva, National Center for Maternal and Child Health, Bishkek, Kyrgyzstan
Email: ak_menta@yahoo.com
Zhaidar S. Saparbekov, Tatyana A. Akmentyeva, Mirbek T. Baizakov, Sultan A. Ormushev, Sagynbek K. Isaev
National Center for Maternal and Child Health, Bishkek, Kyrgyzstan
Abstract
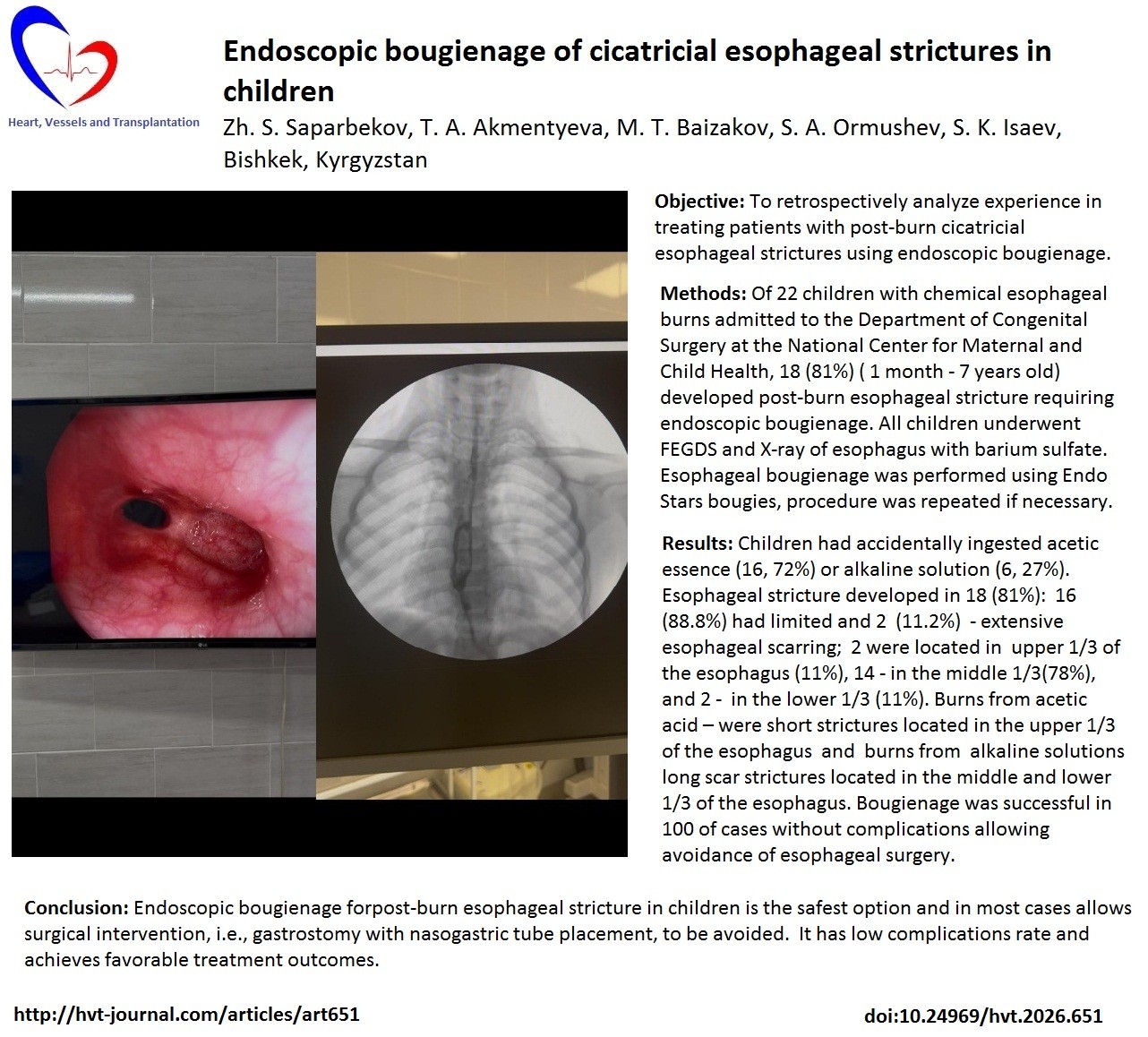
Objective: To retrospectively analyze our experience in treating patients with post-burn cicatricial esophageal strictures using endoscopic bougienage.
Methods: From 2024 to 2025, 22 children aged 1 to 15 years with chemical esophageal burns were admitted to the Department of Congenital Surgery at the National Center for Maternal and Child Health (Bishkek). Post-burn esophageal stricture developed in 18 (81%) (age range 1 month - 7 years old) patients, requiring endoscopic bougienage.. All children underwent FEGDS and X-ray of esophagus with barium sulfate. Esophageal bougienage was performed using Endo Stars bougies, procedure was repeated if necessary. We recorded complications and outcomes of the endoscopic treatment of esophageal strictures.
Results: Children had accidentally ingested acetic essence (16, 72%) or alkaline solution (6, 27%). Esophageal stricture developed in 18 (81%): 16 (88.8%) had limited and 2 (11.2%) - extensive esophageal scarring; 2 were located in upper 1/3 of the esophagus (11%), 14 - in the middle 1/3(78%), and 2 - in the lower 1/3 (11%). Burns from acetic acid – were short strictures located in the upper 1/3 of the esophagus and burns from alkaline solutions long scar strictures located in the middle and lower 1/3 of the esophagus. Endoscopic bougienage proved to be an effective and safe treatment modality for post-burn cicatricial esophageal strictures, allowing avoidance of surgical intervention in 100% of cases.
Conclusion: Endoscopic bougienage for post-burn esophageal stricture in children is the safest option and in most cases allows surgical intervention, i.e., gastrostomy with nasogastric tube placement, to be avoided. It has low complications rate and achieves favorable treatment outcomes.
Key words: Endoscopy, cicatricial stricture, bougienage, esophageal burns, children
Introduction
Esophageal burns are one of the leading causes of esophageal disease and are a serious pathological condition accompanied by profound local and often irreversible systemic changes in the body.
Esophageal burns account for the majority of serious injuries, lead to chronic complications associated with poisoning by toxic substances, and are observed in
18–46% of cases of poisoning by caustic substances in children. Damage to the lips, oropharynx, and upper respiratory tract may also occur.
Chemical burns of the esophagus occur as a result of accidental or intentional (suicidal) ingestion of concentrated acids (vinegar essence, battery electrolyte) or alkalis (ammonia, caustic soda) and other chemically active substances (1, 8).
Graphical abstract
The severity and extent of the burn depend on the nature, amount, and concentration of the chemical substance, the duration of its contact with the mucous membrane, the time elapsed since the injury, as well as individual characteristics of the body and, in part, on emergency care measures (2, 3).
Early consequences of chemical burns of the esophagus include laryngeal edema, exotoxic shock, bleeding, necrosis of the esophageal or gastric wall, mediastinitis, and the formation of cicatricial stenosis. Late complications of include gastroesophageal reflux, hiatal hernia, motility disorders, candidiasis, and malignancy in the long term.
Esophageal scar stenosis is the main problem faced by pediatric surgeons in cases of chemical burns. The outcome of treatment is essentially determined by the nature of the caustic substance. Particularly severe lesions are observed in cases of burns with concentrated alkalis (4).
Currently, the cause of chemical burns of the esophagus in children is accidental ingestion of concentrated solutions of inorganic or organic acids (nitric, sulfuric, hydrochloric, acetic, oxalic), alkali solutions (caustic soda, caustic potash), as well as strong oxidants (potassium permanganate, hydrogen peroxide, other oxidants included in numerous modern detergents, cleaning agents, and bleaching agents) (5).
We use the following classification of esophageal damage (3, 6):
• 0 - no damage
• 1 - erythema and edema
• 2 - non-circular ulceration
• 3 - circular ulceration
• 4 - perforation
There are also more detailed classifications (6):
• Grade 1 - erythema and edema (lesions limited to the superficial layers of the mucosa, possibly with rejection followed by epithelialization without scar formation).
• Grade 2a - vulnerability, hemorrhages, erosions, exudate, blistering (involving the mucosal, submucosal, and muscular layers).
• Grade 2b - same as 2a plus deep or circular ulcers.
• Grade 3a - deep ulcers, “gray or black esophagus” (transmural lesion).
• Grade 3b - extensive necrosis.
Grade 4 - perfortion
According to various authors, scarring due to chemical burns of the esophagus varies widely, ranging from 3% to 74% (1). Today, there are two main approaches to treating patients with post-burn esophageal scarring: minimally invasive interventions (endoscopic methods - balloon dilation, stenting) and surgical reconstruction of the esophagus using various parts of the gastrointestinal tract (2).
Bougienage in various modifications is considered a universally recognized and reliable method of conservative treatment of post-burn esophageal scarring, especially in children. The effectiveness of this procedure is 70-96%. Despite their diversity, the proposed bougienage techniques remain traumatic, and 15-40% of patients experience a recurrence of stricture. The frequency of esophageal perforations during this procedure ranges from 1 to 17.6%. In 11% of cases, bougienage leads to bleeding from the esophagus and stomach, and in 8-10% of cases, it leads to death (6, 7).
The recommended timing for starting esophageal bougienage varies in the literature from 2 days to 1.5 months and remains controversial to this day, and the effectiveness of preventive or early bougienage is assessed ambiguously by different authors (8).
The main advantages of bougienage include its organ-preserving nature, low invasiveness, the possibility of repeated use, faster patient recovery, and a lower incidence of postoperative complications (6, 7).
Research objective: To retrospectively analyze our own experience in treating patients with post-burn cicatricial esophageal strictures using endoscopic dilation.
Methods
Study design and population
The study is descriptive and retrospective analysis experience with endoscopic treatment of esophageal strictures in children.
During the entire observation period from 2024 to 2025, 22 children diagnosed with chemical burns of the esophagus were admitted to the Department of Congenital Malformations Surgery at the National Center for Children’s Health and Development. The inclusion criterion was patients who underwent esophageal dilation as the primary treatment method.
As the study was retrospective no approval of Ethics Committee was required. Informed consent of children parents or guardians was obtained for all procedures. Procedures complied with the Declaration of Helsinki 2024.
Data collection
We recorded age, sex, region of residence, causes of esophageal burns including chemical substances, degrees of esophageal burns, esophageal damage, development of esophageal strictures, their extent (limited or extensive), length (short, medium and long) and location (upper, middle and bottom 1/3rd of esophagus).
Fibroеsophagogastroduodenoscopy and chest X-Ray
Upon admission to the hospital, all children underwent endoscopic and radiological examinations. In the first 24 hours after receiving a chemical burn, it is important for diagnostic purposes to perform an initial fibroеsophagogastroduodenoscopy (FEGDS), which can be used to determine the presence or absence of damage to the esophagus (Fig. 1).
It should be noted that in the first 24 hours after injury, it is very difficult to determine the degree of burn and stricture using endoscopy. Therefore, after comprehensive treatment and relief of the inflammatory process, follow-up FEGDS was performed on the 10th and 21st days after injury to determine the degree of burn.
In order to determine the degree of esophageal narrowing, the length of the stenosis and its diameter, as well as to identify supra-stenotic dilation, X-ray contrast studies of the esophagus with a barium sulfate solution were performed in two projections (Fig. 2).

Figure 1. Narrowing of the esophagus during fibroеsophagogastroduodenoscopy

Figure 2. X-ray contrast examination of the esophagus with barium sulfate
Patient selection for endoscopic bougienage
All patients received antibacterial and comprehensive anti-inflammatory therapy. In addition, sea buckthorn oil and Alma-gel were used as local therapy. Starting from 2024 to 2025, the treatment strategy changed: early preventive bougienage was discontinued. This made it possible to reduce the length of the patient's stay in the hospital: on the 8th–10th day after the inflammatory process was stopped and the general condition improved, and on the 21st day, a follow-up FEGDS was performed on an outpatient basis. A repeat examination was scheduled for 4–6 weeks after the injury, during which an endoscopic examination was performed, resulting in the strict selection of patients with third-degree burns, If scar strictures were detected and in cases of complaints of dysphagia, children were hospitalized.
Endoscopic bougienage
Esophageal dilation was performed in all patients with parental consent. The main bougienage techniques were: 1) blind; 2) with a thread; 3) with a thread, oro-gradient and retrograde; 4) with a metal guide wire; 5) balloon dilatation; 6) endoscopic bougienage.
One of the important aspects in choosing a dilation method is determining the length of the cicatricial stenosis, on which the successful outcome of treatment depends. Depending on the length of the scar stenosis, it is customary to divide it into three types: short (no more than 2.0 cm), extended (from 2.0 to 5.0 cm), subtotal and total strictures (more than 5.0 cm).
Esophageal bougienage was performed using Endo Stars bougies, where the tip of the string consists of an atraumatic spring. The following sizes of guide bougies were used: Fr 5, 7, 9, 11, 13, and 15. This procedure was performed 2–3 times under preoperative sedation in the endoscopy room of the department. After discharge, patients were transferred to outpatient organ dilation according to the standard protocol for all patients with grade III GERD. Esophageal bougienage was discontinued when the esophageal lumen was dilated to 12 mm or more. Bougienage was then performed on an outpatient basis once a week, then once every two weeks.
The criterion for achieving a therapeutic effect in esophageal dilation was a sustained expansion of its lumen to a diameter of 10–12 mm or more, allowing the endoscope to pass freely through the stricture zone, and the free passage of contrast medium through the esophagus, as well as the absence of supra-stenotic dilation during X-ray examination of the organ.
Outcomes
Success of procedures, referral for surgery, complications as bleeding, esophageal perforation, recurrence of stricture and death of children who underwent endoscopic bougienage were recorded.
Statistical analysis
Data are presented as number (%). Data were recorded on Excel software. As the study has a descriptive design no comparative test were performed.
Results
Of the 22 children, 14 were girls (64%) and 8 were boys (36%) aged 1 to 7 years. The age ranges for esophageal burns are shown in Table 1.
|
Table 1. Age range of treated patients with esophageal burns |
|
|
Age |
Number of patients |
|
1 month-1 year 1-3 years 4 – 7 years 7 years and older |
2 10 10 0 |
Of these children, four were admitted to the hospital from the Chui Region (18%); the remaining 18 children were referred from other regions of the Kyrgyz Republic: Jalal-Abad 7 (32%), Osh 6 (27%), Issyk-Kul 2 (9%), Naryn 1 (5%), Batken 1 (5%), and Talas 1 (5%) (Fig. 3).
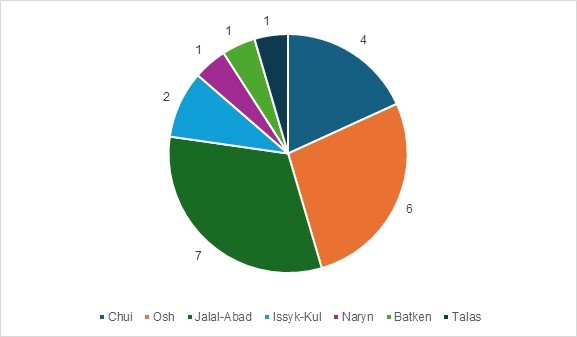
Figure 3. Distribution of incoming children for treatment by region
Among the patients, 4 children had a recent chemical burn of the esophagus (19%), while the remaining 18 presented with post-burn esophageal stricture (81%). Most often, the children who sought treatment had accidentally ingested acetic essence (16, 73%) or alkali (Azelit, anti-fat) (6, 27%). Four children had a first-degree esophageal burn (18%), 12 had a second-degree burn (54%), and 6 had a third-degree esophageal burn (27%). Of the 22 children who sought treatment, post-burn esophageal stricture was subsequently diagnosed in 18 (81%), while 4 had no complications (18%). Sixteen children developed limited esophageal scarring (88.8%), and 2 (11.2%) children developed extensive esophageal scarring. Regarding the location of post-burn esophageal strictures among the 18 children: 2 were in the upper third of the esophagus (11%), 14 in the middle third (78%), and 2 in the lower third (11%).
During the study, it was found that short esophageal strictures are often associated with burns from acetic acid, and the stenosis itself is mainly located in the upper third of the esophagus. Alkaline solutions more often cause long scar strictures, which can be located in the middle and lower thirds of the esophagus.
Endoscopic bougeinage was successful in 100% of cases. There were no complications as bleeding, esophageal perforation, recurrence of stricture and death (nor during procedure or after).
Discussion
Today, issues of early diagnosis, comprehensive therapy, and prevention of possible complications in children with chemical esophageal burns remain relevant. The frequency of scar stenosis of the esophagus after severe chemical burns is quite high and, according to a number of authors, ranges from 8 to 36% (4, 5, 7, 8).
Despite the widespread use of modern methods for diagnosing chemical burns of the esophagus, there are still a fairly significant percentage of diagnostic and tactical errors. In recent years, the number of children with chemical burns of the esophagus has increased, which is associated with the production of new household chemicals, as well as careless storage and use by adults.
The main method for diagnosing chemical burns of the esophagus is endoscopic examination. However, it is very difficult to determine the exact degree of esophageal burns within the first 24 hours after the injury. Therefore, we agree with the authors and believe that follow-up FEGDS on the 10th and 21st days after the injury is a prerequisite for determining the exact extent of organ damage and selecting patients for timely bougienage to prevent the development of esophageal scar stenosis (3). No fatalities were reported during endoscopic dilation.
An analysis of the literature regarding the incidence of postoperative complications and mortality in patients with esophageal strictures caused by scarring who underwent reconstructive surgery suggests that minimally invasive treatment methods, specifically esophageal dilation, are currently the preferred option (7, 8).
Study limitations
The study is limited by small sample size, it retrospective and descriptive nature. Larger prospective studies should on outcomes of endoscopic treatment of esophageal strictures in children should be conducted.
Conclusions
Endoscopic bougienage for post-burn esophageal stricture in children is, in our opinion, the safest option and in most cases allows surgical intervention, i.e., gastrostomy with nasogastric tube placement, to be avoided. It should be noted that the use of endoscopic bougienage for post-burn esophageal stricture in children is not only the safest but also a promising approach that reduces the frequency of complications and achieves favorable treatment outcomes. Thus, dilation of post-burn scar stenosis of the esophagus is an effective and safe treatment method, yielding satisfactory results in both the short-term and long-term periods without resorting to highly invasive surgical treatment.
Ethics: As the study was retrospective no approval of Ethics Committee was required. Informed consent of children parents or guardians was obtained for all procedures. Procedures complied with the Declaration of Helsinki 2024.
Peer-review: External and internal
Conflict of interest: None to declare
Authorship: Zh.S.S., T.A.A., M.T.B., S.A.O. and S.K.I. equally contributed to the study and manuscript preparation. All authors revised and agreed the final version, thus fulfilled authorship criteria.
Acknowledgements and Funding: None to declare.
Statement on A.I.-assisted technologies use: Authors did not use artificial intelligence (A.I.) tools for preparation of manuscript
Data and material availability: Contact authors, any sharing should in frame of fair use an collaboration with acknowledgement of source.
References
| 1. Gavrilik BL, Khmelnitskaya EG, Kiseleva EA, Saley AS. Chemical burns of the esophagus: clinical presentation, diagnosis, psychological aspects. J GrGMU 2007; 4: Available at: URL: https://cyberleninka.ru/article/n/himicheskie-ozhogi-pischevoda-klinika-diagnostika-psihologicheskie-aspekty (accessed: 07.02.2026). | ||||
| 2. Vantsyan EN, Toshchakov RA. Treatment of burns and scar narrowing of the esophagus. Moscow: Medicine; 1971. 260 p. | ||||
| 3. UptoDate. Available at: URL: https://www.uptodate.com/contents/caustic-esophageal-injury-in-children/contributors May 30, 2025. | ||||
| 4. Razumovsky AYu, Geraskin AV, Obydennova RV, Kulikova NV. Treatment of chemical burns of the esophagus in children. Surgery J named after N.I. Pirogov 2012; 1: 43-8. | ||||
| 5. Nuutinen M, Uhari M, Karvali T, Kouvalainen K. Consequences of ingesting caustic substances in children. Acta Paediatr 1994; 83: 1200. https://doi.org/10.1111/j.1651-2227.1994.tb18281.x PMid:7841737 |
||||
| 6. Zargar SA, Kochhar R, Mehta S, Mehta SK. The role of fiberoptic endoscopy in the treatment of caustic poisoning and a modified endoscopic classification of burns. Gastrointest Endosc 1991; 37:165. https://doi.org/10.1016/S0016-5107(91)70678-0 PMid:2032601 |
||||
| 7. Sharipov AM, Shamszoza HA, Rakhmatova RA, Yusupov BKh, Dodochonov YuT, Sayfulloyev AA, et al. Treatment of children with the consequences of chemical burns of the esophagus. Russ J Pediatr Surg Anesth Resusc 2020; 10: 217-26. doi: 10.17816/psaic678 https://doi.org/10.17816/psaic678 |
||||
| 8. Voskresenskaya ML, Plekhanov AN. Results of treatment of chemical burns and post-burn strictures of the esophagus (literature review). Acta Biomed Scient 2015; 5 :107-12. | ||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
