Aslanger’s pattern in non-ST-elevation myocardial infarction: Prevalence and angiographic correlates in a Vietnamese single-center cohort
ORIGINAL RESEARCH ARTICLE
Aslanger’s pattern in non-ST-elevation myocardial infarction: Prevalence and angiographic correlates in a Vietnamese single-center cohort
Article Summary
- DOI: 10.24969/hvt.2026.658
- CARDIOVASCULAR DISEASES
- Published: 19/06/2026
- Received: 28/04/2026
- Revised: 08/06/2026
- Accepted: 08/06/2026
- Views: 15
- Downloads: 8
- Keywords: Aslanger’s pattern, NSTEMI, electrocardiography, coronary angiography, right coronary artery, multivessel disease
Address for Correspondence: Binh Thi Thanh Dao, Department of Medicine, HUTECH University, Ho Chi Minh City, Vietnam
Email: dtt.binh@hutech.edu.vn Phone: +84 913 704 458
ORCID: Binh Thi Thanh Dao - 0009-0006-1428-9206; Minh Quang Nguyen - 0009-0006-7836-5212;
Anh Do Nguyen - 0009-0003-0631-1555
Binh Thi Thanh Dao1, Minh Quang Nguyen2, Anh Do Nguyen2
1Department of Medicine, HUTECH University, Ho Chi Minh City, Vietnam
2Department of Interventional Cardiology, Nhan Dan Gia Dinh Hospital, Ho Chi Minh City, Vietnam
Abstract
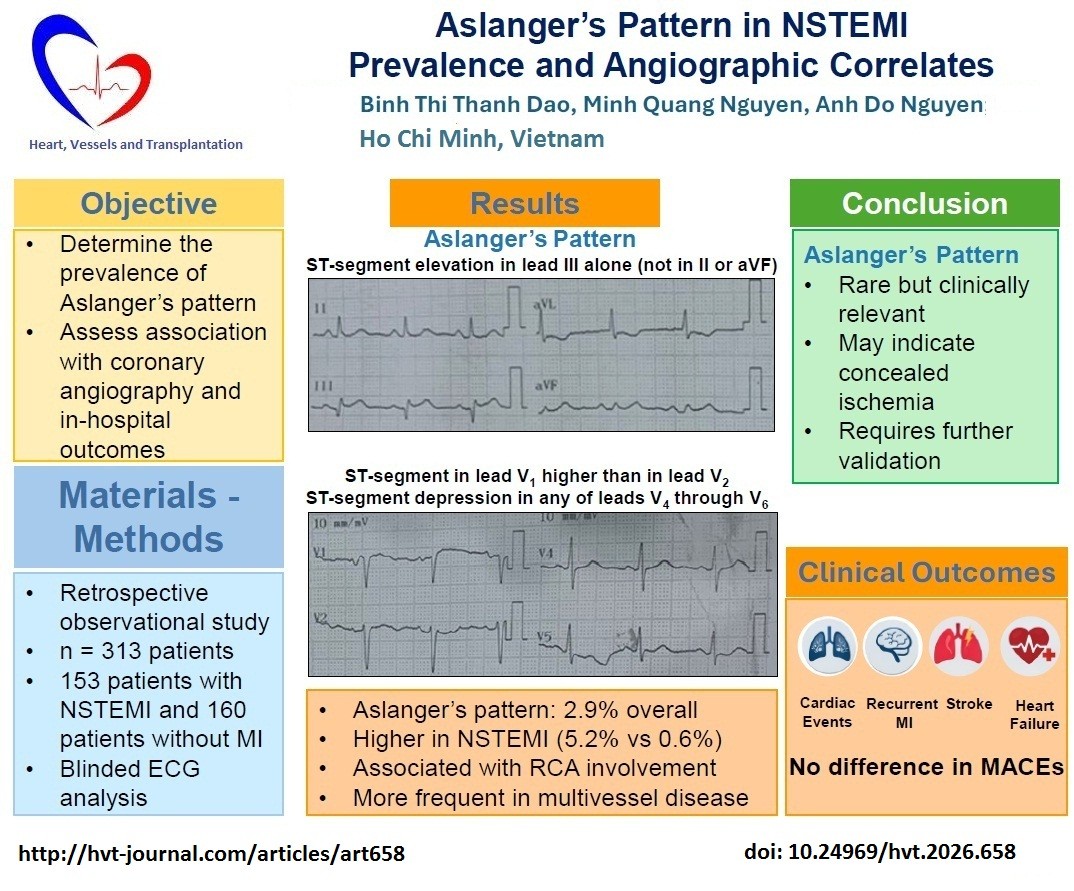
Objective: Aslanger’s pattern is a recently described electrocardiographic sign that may indicate inferior myocardial ischemia in the absence of classic ST-segment elevation, potentially leading to under-recognition in patients with acute coronary syndrome (ACS). However, its prevalence and angiographic correlates remain poorly characterized, particularly in Southeast Asian populations.
The objective of the study was to determine the prevalence of Aslanger’s pattern and to explore its association with coronary angiographic findings and in-hospital outcomes among patients undergoing coronary angiography for suspected ACS.
Methods: This retrospective single-center study included 313 patients (153 non-ST-elevation myocardial infarction [NSTEMI], 160 without myocardial infarction) at a Vietnamese tertiary hospital. Admission electrocardiograms were independently reviewed by two blinded cardiologists using predefined criteria. Coronary angiographic characteristics, including culprit vessel involvement and the presence of multivessel disease, were analyzed.
Results: Aslanger’s pattern was identified in 9 patients (2.9%), including 8 patients in the NSTEMI group (5.2%) and 1 patient in the non-myocardial infarction group (0.6%). Among all cases in the NSTEMI group who exhibited the Aslanger’s pattern, there was right coronary artery involvement and multivessel disease. Due to the small number of events, formal statistical comparisons were limited. In-hospital adverse events were infrequent, and no robust differences were observed between groups.
Conclusion: In this cohort, Aslanger’s pattern was uncommon but appeared more frequent in NSTEMI patients and was associated with right coronary artery involvement and multivessel disease. Given the small sample size, these findings should be considered hypothesis-generating. Larger multicenter studies are required to validate their diagnostic and prognostic significance.
Key words: Aslanger’s pattern, NSTEMI, electrocardiography, coronary angiography, right coronary artery, multivessel disease
![]()
Graphical abstract
List of abbreviations
ACS- acute coronary syndrome
ECG- electrocardiogram
LAD- left anterior descending artery
MACE- major adverse cardiovascular events
MI- myocardial infarction
MVD- multivessel disease
NSTEMI- non-ST-elevation myocardial infarction
RCA- right coronary artery
Introduction
The traditional classification of acute coronary syndrome (ACS) into ST-elevation myocardial infarction (STEMI) and non-ST-elevation myocardial infarction (NSTEMI) is increasingly scrutinized. Emerging evidence suggests that approximately 25% of patients diagnosed with NSTEMI actually harbor a total acute coronary occlusion (1, 2). These patients, often categorized as "OMI" (Occlusion Myocardial Infarction), suffer from delayed revascularization, leading to larger infarct sizes and higher mortality rates compared to true NSTEMI (3).
The 12-lead electrocardiogram (ECG) is the primary tool for triage, yet it lacks sensitivity for certain territories or when multiple ischemic vectors coexist (4). In 2020, Emre Aslanger and colleagues identified a new ECG pattern indicating inferior myocardial infarction in the presence of multivessel disease (MVD) (5). This pattern is characterized by ST-segment elevation isolated to lead III, which is often misinterpreted or overlooked as a non-specific change.
In regions like Southeast Asia, where the prevalence of metabolic syndrome and late clinical presentation is high, the incidence of MVD is significant (6, 7). Understanding the diagnostic value of Aslanger’s pattern in this specific population is vital.
This study evaluates the prevalence of Aslanger’s pattern and its association with angiographic severity and in-hospital clinical outcomes among patients undergoing coronary angiography for suspected ACS.
Methods
Study design and setting
This was a retrospective single-center observational study conducted at the Vietnamese tertiary hospital. Consecutive patients presenting with suspected ACS between August 2019 and February 2022 were screened for eligibility.
Study population
During the study period, a total of 391 consecutive patients with suspected ACS were assessed for eligibility. Patients with a prior history of myocardial infarction (n = 36), previous coronary revascularization (percutaneous coronary intervention [PCI] or coronary artery bypass surgery [CABG]; n=23), or pacemaker rhythm or uninterpretable ECGs (n=19) were excluded. No patients were excluded because of incomplete clinical or angiographic data. The final study population comprised 313 patients, including 153 patients with NSTEMI and 160 control subjects in whom acute myocardial infarction was excluded by serial cardiac troponin measurements, repeated ECG assessment, and final discharge diagnosis. Patients were included in the NSTEMI group diagnosed according to the Fourth Universal Definition of Myocardial Infarction (1). A control group (non-myocardial infarction [MI] group) included symptomatic patients without MI, defined by normal serial troponin levels and absence of dynamic ischemic ECG changes, with an alternative diagnosis established at discharge (Fig. 1).
The study protocol was reviewed and approved by local institutional ethics committee for Biomedical Research of, under certificate, dated March 8, 2022. Informed consent was waived due to the retrospective design. Patient anonymity: All clinical data and ECG/angiographic images were fully anonymized. No identifiable patient information is included in this manuscript. The study was performed in compliance with Helsinki 2024 rules for human studies.
Baseline variables
Baseline variables included age, sex, hypertension, diabetes mellitus, current smoking, heart rate, systolic blood pressure, and admission troponin levels.
ECG analysis and interpretation
All admission 12-lead ECGs (25 mm/s, 10 mm/mV) were analyzed by two independent cardiologists blinded to the angiographic results. Discrepancies were resolved by a third senior consultant. Interobserver agreement was planned to be assessed using Cohen’s kappa statistic; however, the original reader-level classification matrix was not available for retrospective calculation. Aslanger’s pattern was diagnosed based on the following triad (5, 8):
1. ST-segment elevation in lead III alone (not in II or aVF).
2. ST-segment depression in any of leads V4 through V6 (with a positive or terminal positive T-wave), but not in lead V2.
3. ST-segment in lead V1 higher than in lead V2.
Coronary angiography
All NSTEMI patients underwent coronary angiography within 24–48 hours in accordance with guideline-based practice (4). The angiographic variables collected, including coronary artery involvement, number of diseased vessels, and MVD. Significant stenosis was defined as ≥70% luminal narrowing (≥50% for the left main artery). Multivessel disease was defined as significant stenosis of two or more major epicardial coronary arteries.
Clinical outcomes
In-hospital major adverse cardiovascular events (MACEs) included cardiovascular death, recurrent MI, heart failure, and stroke. Analyses were descriptive due to low event rates.
Statistical analysis
Statistical analyses were performed using Stata 17.0/IC software for Mac (TX: StataCorp LP). Continuous variables are presented as mean (standard deviation) for normally distributed data or as median with interquartile range (IQR) for skewed distributions.
Comparisons between groups were performed using the independent-samples t test for normally distributed variables (age, heart rate, and systolic blood pressure) and the Mann–Whitney U test for non-normally distributed variables (high-sensitivity cardiac troponin T).
Categorical variables are expressed as counts and percentages. Because of the low prevalence of Aslanger’s pattern, Fisher’s exact test was used for categorical comparisons.
Owing to the limited number of patients with Aslanger’s pattern, multivariable analysis was not considered statistically reliable and was therefore not performed. All analyses were considered exploratory and hypothesis-generating.
Results
Baseline characteristics
A total of 313 patients were included, comprising 153 NSTEMI patients and 160 non-MI patients (Fig. 1).
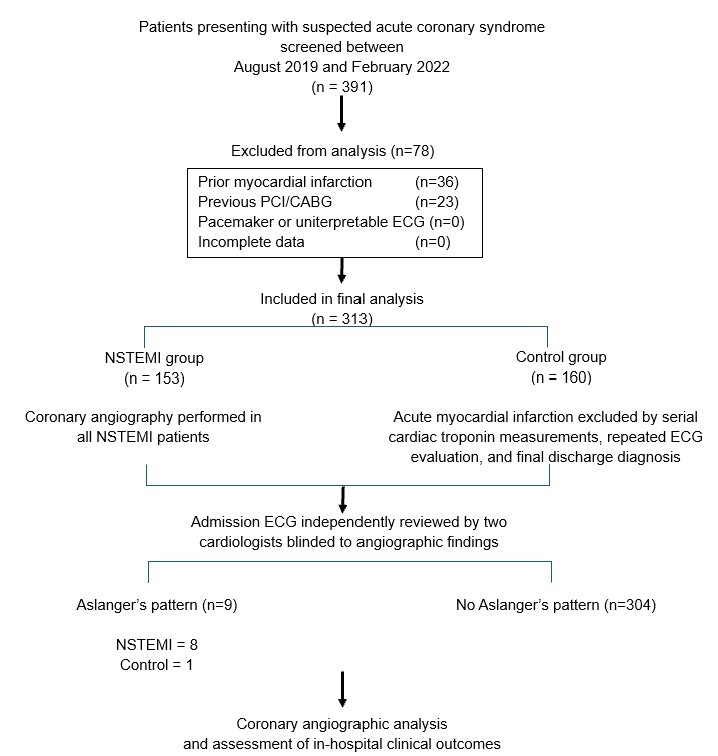
Figure 1. Study flow diagram
The mean age of patients was 63.4 years, with a predominance of male patients (65.8%). NSTEMI patients were younger (p=0.035), had a higher prevalence of diabetes (p=0.021), higher admission heart rates and hs-TnT levels (both p<0.001) as compared to control group (Table 1).
Prevalence of Aslanger’s Pattern
Aslanger’s pattern was identified in 9 patients (2.9%), including 8 NSTEMI patients (5.2%) and 1 non-MI patient (0.6%) (Table 1, p=0.015). A representative case illustrating the electrocardiographic features of this pattern is shown in Figure 2.
|
Table 1. Baseline clinical and laboratory characteristics of the study population |
|||
|
Variables |
NSTEMI Group (n=153) |
Non-MI Group (n=160) |
p |
|
*Age, years |
63.0 (10.0) |
65.6 (11.5) |
0.035 |
|
Male gender, n(%) |
95 (62.1) |
89 (55.6) |
0.246 |
|
Medical history, n(%) |
|||
|
Hypertension |
108 (70.6) |
119 (74.4) |
0.453 |
|
Diabetes mellitus |
64 (41.8) |
47 (29.4) |
0.021 |
|
Current smoking |
54 (35.3) |
45 (28.1) |
0.173 |
|
Physical and laboratory findings |
|||
|
*Heart rate, bpm |
88.0 (17.7) |
80.2 (13.2) |
<0.001 |
|
*Systolic BP, mmHg |
136.2 (23.4) |
139.8 (22.8) |
0.170 |
|
**hs-TnT, pg/mL |
818.5 (229-1300) |
7.5 (5-13) |
<0.001 |
|
Aslanger’s pattern |
8 (5.2) |
1 (0.6) |
0.015 |
|
Data are presented as *mean (SD), **median (IQR), or number (%), as appropriate. Continuous variables were compared using the independent-samples t test or the Mann–Whitney U test according to data distribution. Categorical variables were compared using the Chi-square test or Fisher's exact test, as appropriate BP – blood pressure, bpm- beats per minute, hs-TnT – high sensitive troponin, IQR – interquartile range, MI – myocardial infarction, NSTEMI – non-ST-elevation MI |
|||
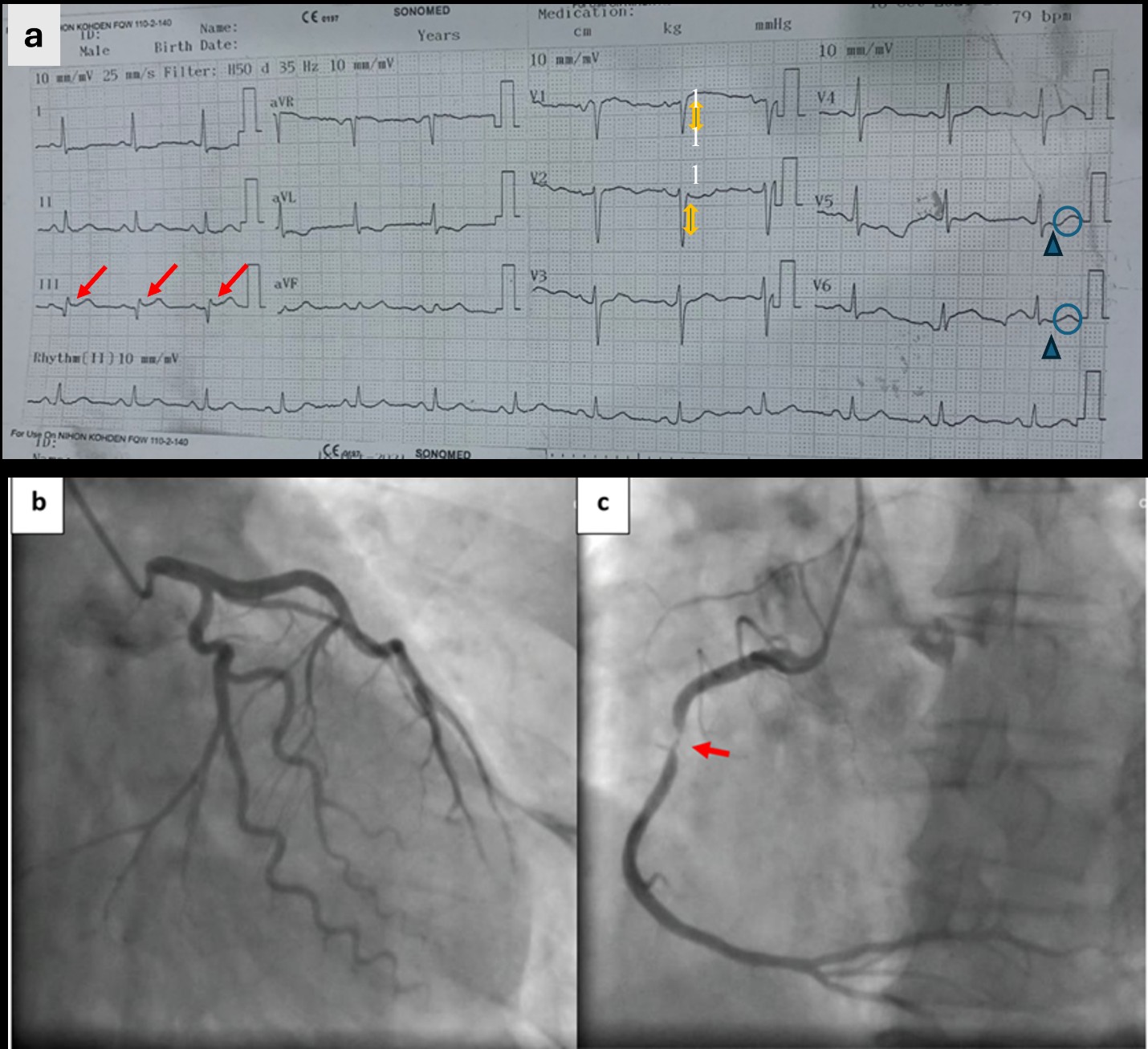
Figure 2. Representative case of Aslanger’s pattern associated with significant right coronary artery stenosis.
(a)Admission 12-lead electrocardiogram (ECG) demonstrating the Aslanger’s pattern, characterized by isolated ST-segment elevation in lead III without elevation in other inferior leads (II or aVF), accompanied by ST-segment depression in lead I and across precordial leads V4–V6 with a positive T-wave in lead V1; (b) Baseline coronary angiography showing a normal left coronary artery (LCA) system; (c) Selective angiography of the right coronary artery (RCA) revealing a 95% obstructive stenosis in the mid-segment (arrow), confirming the presence of an occlusion myocardial infarction despite the absence of traditional STEMI criteria.
Angiographic findings
Among NSTEMI patients, those with Aslanger’s pattern had a higher frequency of RCA involvement (100% vs. 64.8%) and multivessel disease (100% vs. 71.7%) (both p=0.04). These findings should be interpreted cautiously due to small sample size (Table 2).
Clinical Outcomes
In-hospital events were infrequent. No meaningful differences in outcomes as heart failure of MACE were observed between groups, and the study was not powered for outcome analysis (Table 2).
|
Table 2. Angiographic characteristics and in-hospital outcomes in NSTEMI patients |
|||
|
Variables |
Aslanger’s (+) (n=8) |
Aslanger’s (–) (n=145) |
p |
|
Coronary involvement, n (%) |
|||
|
Right coronary artery (RCA) |
8 (100.0) |
94 (64.8) |
0.040 |
|
Left anterior descending (LAD) |
4 (50.0) |
122 (84.1) |
0.014 |
|
Left circumflex (LCX) |
5 (62.5) |
73 (50.3) |
0.495 |
|
Extent of Disease, n (%) |
|||
|
Multivessel disease |
8 (100.0) |
104 (71.7) |
0.040 |
|
In-hospital Outcomes, n (%) |
|||
|
Heart Failure |
2 (25.0) |
23 (15.9) |
0.496 |
|
Major adverse events (MACE)* |
0 (0.0) |
2 (1.4) |
0.738 |
|
Data are presented as number (%) Fischer exact test *MACE includes cardiac death, recurrent MI, and stroke, NSTEMI – non-ST-elevation myocardial infarction |
|||
Discussion
Main findings
In this retrospective single-center study, Aslanger's pattern was identified in a small proportion of patients with NSTEMI (5.2%) and was rarely observed among patients without MI. All NSTEMI patients exhibiting this ECG pattern demonstrated RCA involvement and multivessel coronary artery disease on coronary angiography. Because of the limited number of cases, these findings should be interpreted as exploratory and hypothesis-generating; nevertheless, they support the potential clinical value of recognizing Aslanger's pattern in patients presenting with suspected ACS.
Electrophysiological mechanisms
The most profound aspect of Aslanger’s pattern lies in the concept of "vector cancellation." In a standard inferior STEMI, the ST-segment elevation vector is directed inferiorly and slightly to the right (toward lead III) or left (toward lead II) (9). However, when concomitant diffuse subendocardial ischemia occurs, typically due to MVD or left main insufficiency, an additional ST-segment vector is generated, directed toward the left and superiorly (leads I, aVL, V4-V6) (3, 10).
These two vectors interact: the superior-leftward vector of subendocardial ischemia pulls the inferior elevation vector away from leads II and aVF. Because lead III (+1200) is the most rightward of the inferior leads, the ST-elevation remains visible only in lead III (3, 10). Our findings of 100% RCA involvement and 100% MVD in patients with Aslanger’s pattern directly support this electro-vectoral theory.
Comparison with other NSTEMI patterns
Aslanger’s pattern should be differentiated from other "STEMI-equivalents" such as the de Winter pattern (associated with proximal LAD occlusion) or the Wellens’ syndrome (11, 12). Unlike de Winter, which signifies anterior ischemia, Aslanger points specifically to the inferior territory. In our study, the high specificity for RCA involvement suggests that Aslanger’s pattern is not merely a marker of "severe disease" but a precise anatomical indicator.
Clinical and prognostic significance in Vietnam
The prevalence of Aslanger's pattern observed in our study was broadly consistent with the limited available literature, which generally suggests that this ECG pattern is uncommon among patients presenting with ACS (5). Variability between studies should be interpreted cautiously, as reported frequencies may be influenced by differences in inclusion criteria, patient characteristics, referral patterns, and sample size. In addition, because Aslanger's pattern was only recently described, the available evidence remains relatively sparse, limiting direct comparisons across populations.
A representative electrocardiographic example of Aslanger's pattern is shown in Figure 2.
Our study observed a heart failure rate of 25% in patients with Aslanger’s pattern. While this did not reach statistical significance due to the small sample size, it underscores the severity of the pattern. In clinical practice, many of these patients might be delayed for angiography because they do not meet "STEMI criteria" (3). However, given the 100% prevalence of MVD and RCA disease found here, we argue that Aslanger’s pattern may help identify a subgroup of NSTEMI patients with a high likelihood of RCA involvement and multivessel disease, warranting heightened clinical attention and further validation in larger cohorts.
The study period partially overlapped with the COVID-19 pandemic, which may have affected healthcare utilization and admission patterns for ACS. However, these factors were not systematically evaluated and therefore could not be formally analyzed.
Study limitations
This study has several limitations. First, the number of patients with Aslanger’s pattern was very small, the possible influence of the COVID-19 pandemic on healthcare utilization during the study period, limiting statistical power and precluding reliable multivariable adjustment. Second, the study was conducted at a single tertiary referral center, which may have enriched the population for more severe coronary disease and reduced generalizability. Third, the retrospective design carries an inherent risk of selection and information bias. Fourth, the control group was clinically useful for estimating overall prevalence but is less informative than an internal comparison between NSTEMI patients with and without the pattern when addressing angiographic correlates. Finally, the study was not powered to assess clinical outcomes.
Conclusion
Aslanger’s pattern was infrequent in this Vietnamese single-center cohort but appeared more common in NSTEMI than in control patients. Among patients with NSTEMI, the pattern was associated with significant RCA involvement and multivessel disease. These findings support the potential diagnostic relevance of this ECG sign, although larger multicenter studies are required before firm clinical recommendations can be made.
Ethics: The study protocol was reviewed and approved by local institutional ethics committee for Biomedical Research of, under certificate, dated March 8, 2022. Informed consent was waived due to the retrospective design. Patient anonymity: All clinical data and ECG/angiographic images were fully anonymized. No identifiable patient information is included in this manuscript. The study was performed in compliance with Helsinki 2024 rules for human studies.
Peer-review: External and internal
Conflict of interest: The authors declare that they have no competing interests.
Authorship: B.T.T.D., M.Q.N., and A.D.N. equally contributed to manuscript preparation and fulfilled authorship criteria.
Acknowledgements: The authors thank the staff of the hospital for their support in data collection and patient care.
Funding: None to declare.
Statement on A.I.-assisted technologies use: Artificial intelligence-assisted tools were used solely for language editing and improvement of manuscript readability. The authors reviewed and verified all scientific content and take full responsibility for the accuracy and integrity of the work.
Data and material availability: The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request. Any share should be in frame of fair use with acknowledgement of source and/collaboration.
References
| 1.Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA. Fourth universal definition of myocardial infarction (2018).Eur Heart J 2019; 40: 237-69. https://doi.org/10.1093/eurheartj/ehy856 https://doi.org/10.1093/eurheartj/ehy462 PMid:30165617 |
||||
| 2.Khan AR, Golwala H, Tripathi A, et al. Impact of total occlusion of culprit artery in acute non-ST elevation myocardial infarction: a systematic review and meta-analysis. Eur Heart J 2017; 38: 3082-9. doi:10.1093/eurheartj/ehx418 https://doi.org/10.1093/eurheartj/ehx418 PMid:29020244 |
||||
| 3.Meyers HP, Bracey A, Lee D, et al. Comparison of the ST-elevation myocardial infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of acute myocardial infraction. J Emerg Med 2021; 60: 273-84. doi:10.1016/j.jemermed.2020.10.026 https://doi.org/10.1016/j.jemermed.2020.10.026 PMid:33308915 |
||||
| 4.Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J 2023; 44: 3720-826. doi:10.1093/eurheartj/ehad191 https://doi.org/10.1093/eurheartj/ehad191 PMid:37622654 |
||||
| 5.Aslanger E, Yıldırımtürk Ö, Şimşek B, et al. A new electrocardiographic pattern indicating inferior myocardial infarction. J Electrocardiol 2020; 61: 41-6. doi:10.1016/j.jelectrocard.2020.04.008 https://doi.org/10.1016/j.jelectrocard.2020.04.008 PMid:32526537 |
||||
| 6.Isezuo S, Subban V, Krishnamoorthy J, et al. Characteristics, treatment and one-year outcomes of patients with acute coronary syndrome in a tertiary hospital in India. Indian Heart J 2014; 66: 156-63. doi:10.1016/j.ihj.2013.12.023 https://doi.org/10.1016/j.ihj.2013.12.023 PMid:24814108 PMCid:PMC4017571 |
||||
| 7.Sidhu NS, Rangaiah SKK, Ramesh D, Veerappa K, Manjunath CN. Clinical characteristics, management strategies, and in-hospital outcomes of acute coronary syndrome in a low socioeconomic status cohort: An observational study from urban India. Clin Med Insights Cardiol 2020; 14: 117954682091889. doi:10.1177/1179546820918897 https://doi.org/10.1177/1179546820918897 PMid:32425627 PMCid:PMC7218326 |
||||
| 8.Miyauchi E, Kuwazuru K, Arikawa R, et al. Clinical features of the Aslanger pattern to compensate for the limitation of ST-elevation myocardial infarction (STEMI) criteria. Cureus 2023; doi:10.7759/cureus.33227 https://doi.org/10.7759/cureus.33227 |
||||
| 9.Birnbaum Y, Rankinen J, Jneid H, Atar D, Nikus K. The role of ECG in the diagnosis and risk stratification of acute coronary syndromes: an old but indispensable tool. Curr Cardiol Rep 2022; 24: 109-118. doi:10.1007/s11886-021-01628-7 https://doi.org/10.1007/s11886-021-01628-7 PMid:35028816 |
||||
| 10.Aslanger EK, Yıldırımtürk Ö, Şimşek B, et al. DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardial infarction (DIFOCCULT Study). Int J Cardiol Heart Vasc 2020; 30: 100603. doi:10.1016/j.ijcha.2020.100603 https://doi.org/10.1016/j.ijcha.2020.100603 PMid:32775606 PMCid:PMC7399112 |
||||
| 11.de Winter RJ, Verouden NJW, Wellens HJJ, Wilde AAM, Interventional Cardiology Group of the Academic Medical Center. A new ECG sign of proximal LAD occlusion. N Engl J Med 2008; 359: 2071-3. doi:10.1056/NEJMc0804737 https://doi.org/10.1056/NEJMc0804737 PMid:18987380 |
||||
| 12.Al-assaf O, Abdulghani M, Musa A, AlJallaf M. Wellen's syndrome. Circulation 2019; 140: 1851-2. doi:10.1161/CIRCULATIONAHA.119.043780 https://doi.org/10.1161/CIRCULATIONAHA.119.043780 PMid:31765255 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
