Viability beyond remodeling: Chronic total occlusion PCI in a patient with refractory angina and improved LV function
CASE REPORT
Viability beyond remodeling: Chronic total occlusion PCI in a patient with refractory angina and improved LV function
Article Summary
- DOI: 10.24969/hvt.2026.661
- CARDIOVASCULAR DISEASES
- Published: 19/06/2026
- Received: 15/04/2026
- Revised: 15/05/2026
- Accepted: 15/05/2026
- Views: 21
- Downloads: 8
- Keywords: Chronic total dysfunction, left ventricular remodeling, left ventricular dysfunction, percutaneous coronary intervention, stenting, outcome
Address for Correspondence: Randa Tabbah, Division of Cardiology, Holy Spirit of Kaslik University, Notre Dame de Secours University Hospital; Division of Cardiology, St John University Hospital, Lebanese American University; Division of Cardiology, Balamand University, Notre Dame du Liban University Hospital, Beirut, Lebanon
Email: randa_22tabbah@hotmail.com
ORCID: Randa Tabbah - 0000-0003-2987-9568 Twitter: @22tabbah_randa
Facebook: Randa Tabbah - @randa.tabbah, Bassam Harb - @bassam.harb, Karam Karam - @karam.karam
Randa Tabbah1a,2,3, Bassam Harb 1,2, Karam Karam4b
1aDivision of Cardiology and 1bDivision of Cardiothoracic Surgery, Holy Spirit of Kaslik University, Notre Dame de Secours University Hospital, Beirut, Lebanon
2Division of Cardiology, St John University Hospital, Lebanese American University, Beirut, Lebanon
3Division of Cardiology, Balamand University, Notre Dame du Liban University Hospital, Beirut, Lebanon
Abstract
Objective: Chronic total occlusion (CTO) remains a challenging subset in interventional cardiology, particularly in patients with left ventricular dysfunction. The optimal timing of revascularization in the presence of myocardial viability and ongoing reverse remodeling remains controversial.
Case presentation: We report the case of a 35-year-old patient with a previously unrecognized myocardial infarction presenting with severe ventricular dysfunction (ejection fraction [EF] 20%), functional mitral regurgitation (MR), and a right coronary artery CTO. Following guideline-directed medical therapy (GDMT), significant improvement was observed at 3 months, with EF increasing to 41% and MR decreasing from moderate–severe to mild–moderate, consistent with reverse remodeling. Despite this recovery, persistent symptoms and evidence of myocardial viability prompted a second attempt for revascularization. Successful percutaneous coronary intervention was achieved with drug-eluting stent implantation, restoring TIMI III flow.
This case highlights the role of myocardial viability and reverse remodeling in guiding CTO revascularization. It supports a deferred, stepwise strategy in selected patients, allowing initial recovery under GDMT before intervention. Improvement in functional MR paralleled ventricular geometric restoration, emphasizing its dynamic and secondary nature.
Conclusion: In young patients with ischemic cardiomyopathy, delayed CTO revascularization following medical optimization may enhance outcomes. A personalized strategy integrating symptoms, viability, and ventricular remodeling is essential for optimal management.
Key words: Chronic total dysfunction, left ventricular remodeling, left ventricular dysfunction, percutaneous coronary intervention, stenting, outcome
(Heart Vessels Transplant 2026: 10: doi:10.24969/hvt.2026.661)
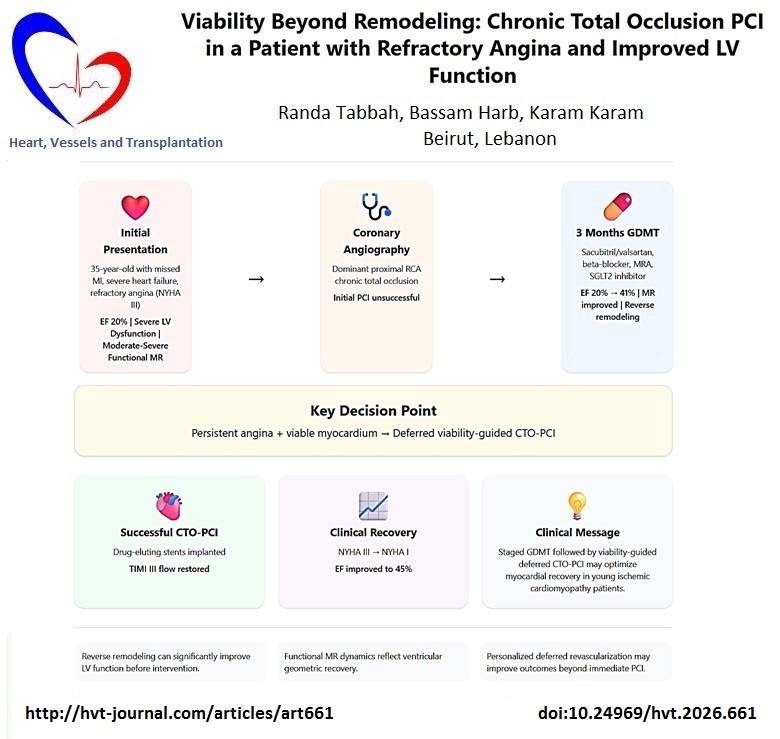
![]()
Graphical abstract
Introduction
Chronic total occlusion (CTO) of a coronary artery remains one of the most challenging scenarios in interventional cardiology, both technically and in terms of clinical decision-making (1). While advances in percutaneous coronary intervention (PCI) techniques have improved success rates, the indication for CTO revascularization—particularly in the setting of left ventricular (LV) dysfunction—remains debated (2).
The presence of myocardial viability within the CTO territory has emerged as a key determinant in selecting patients who may derive prognostic and symptomatic benefit from revascularization (2). Furthermore, the interplay between ischemic cardiomyopathy, secondary mitral regurgitation (MR), and ventricular remodeling introduces an additional layer of complexity. Functional MR in this context is highly dynamic and closely related to LV geometry, papillary muscle displacement, and tethering forces (3).
We report a case of a young patient with a previously unrecognized myocardial infarction leading to severe LV dysfunction, functional MR, and a CTO of the right coronary artery (RCA), who demonstrated significant spontaneous recovery of LV function under optimal medical therapy.
This case highlights the role of delayed revascularization in the presence of myocardial viability and explores the mechanisms underlying reverse remodeling and MR improvement.
Case report
A 35-year-old patient presented with dyspnea New York Heart Association (NYHA class III), and chest pain on exertion. He was known to have a history of myocardial infarction that was misdiagnosed as indigestion. He was diagnosed when he was presented 2 months later with heart failure and pulmonary congestion.
Informed written consent was obtained from patients for all procedures and treatment. The case was managed in a compliance with Helsinki 2024 agreement on human studies.
A cardiac ultrasound was done, which revealed an ejection fraction (EF) of 20% and a longitudinal strain of -6%, high LV end-diastolic pressure, and moderate to severe eccentric MR with Coanda effect, moderate right ventricular dysfunction with moderate tricuspid regurgitation and increased systolic pulmonary pressures at 50mmHg (Fig 1). An electrocardiogram (ECG) revealed a pseudo-Q wave in the inferior leads, a sign of old myocardial infarction (Fig 2).
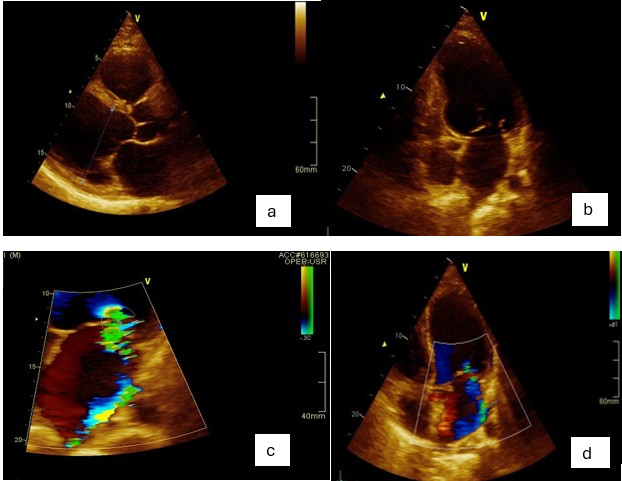
Figure 1. A) Parasternal long axis view revealing a dilated left ventricle; B) 4-chamber/2-chamber view with inferobasal hypokinesis and deformation; C) A zoomed view of the left atrium with an eccentric mitral regurgitation reaching the roof of the left atrium and the pulmonary veins; D) 4-chamber view with color Doppler on the mitral valve
Cardiac catheterization presented a dominant, totally occluded RCA proximally with small collaterals from the left anterior descending artery (LAD). An attempt to revascularize the RCA wasn’t successful, and the patient was discharged on guidelines-directed medical therapy (GDMT) for heart failure (sacubitril valsartan 200 mg twice daily, empagliflozin 10 mg daily, eplerenone 25mg once daily, carvedilol 12.5mg daily, clopidogrel 75mg daily and furosemide 20mg daily).
After 3 months of medical therapy, he presented to our institution for cardiac evaluation. A cardiac ultrasound was done, revealing an improved EF of 41% with inferobasal and inferolateral hypokinesis, but not akinesis and an improved MR due to tethering of the posterior mitral leaflet with an eccentric jet not reaching the pulmonary veins anymore, with grade I-II.
The improvement in MR is possibly due to a reverse ventricular remodeling, which reduces the apical displacement of the papillary muscles and reduces leaflet tethering. With the restoration of better LV geometry, the tension on the chordae is reduced, allowing the leaflets to regain better coaptation.
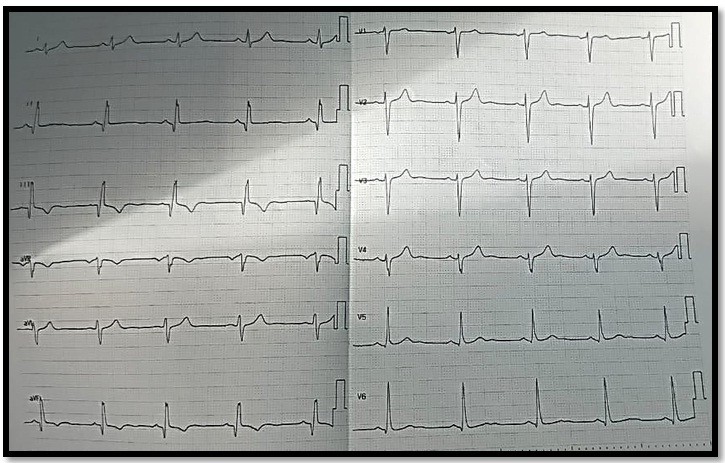
Figure 2. Electrocardiogram showing pseudo Q wave in inferior leads
Despite improvement in his LV function, the patient still has symptoms of dyspnea and chest pain, and there is still viability in the RCA territory with small collaterals. We opted for a reattempt to revascularize the RCA (Fig. 3). A coronary angioplasty was performed via the left radial artery using JR 3.5 guiding catheter. The RCA was crossed with a Fielder XTA wire. Pre-dilatation was done using first a Ryurei 1.25x20 up to 16 atmospheres, then a Mini Trek 2.0 x2 0 up to 18 atmospheres. A Xience SkyPoint stent, 3.5x38, was successfully placed in the distal RCA after being inflated to 16 atmospheres for 20 seconds. Another stent, 3.5x48 (overlapped to the already implanted one), was placed in the proximal-mid RCA. Post-dilatation was done using a non-compliant balloon, NC trek 3.5x20 at 20 atmospheres. Excellent result with no dissection and a TIMI III flow, blush grade 3 was achieved. The RCA is dominant and huge, extending to the apex of the heart.
Figure 3 provides an idea of the morphology of the RCA before and after CTO.
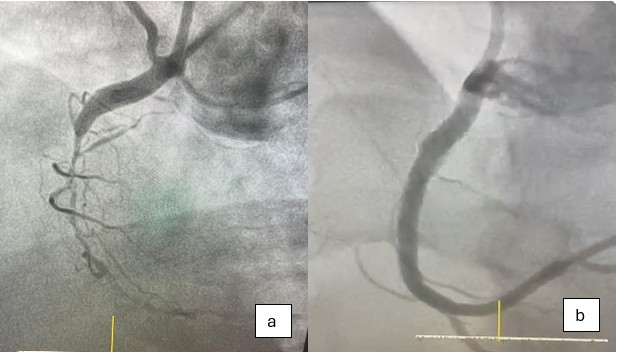
Figure 3. A) Before angioplasty: CTO of the RCA; B) After angioplasty: Reperfusion with TIMI III flow
CTO – chronic total occlusion, RCA- right coronary artery
He was discharged on dual antiplatelets: ticagrelor and aspirin for 12 months in addition to heart failure medication with close follow-up. At follow-up in 3 months, the patient was free of chest pain with improvement of dyspnea (NYHA class I). Improvement in EF was also noticed =45% with improvement in the inferobasal wall kinesis.
Discussion
This case illustrates several important and evolving concepts in the management of ischemic cardiomyopathy with CTO.
Spontaneous reverse remodeling under medical therapy
One of the most striking features in this case is the significant improvement in LV EF (from 20% to 41%) within three months of GDMT. This suggests the presence of stunned or hibernating myocardium rather than irreversible scar. Thus spontaneous reverse remodeling is possible on medical therapy (4). The observed improvement supports the concept that early aggressive medical therapy alone may lead to partial functional recovery, even in the presence of a CTO. This raises an important clinical question: Should CTO revascularization be sometimes delayed allowing for myocardial recovery under GDMT? In selected patients, especially younger individuals with recent ischemic injury, a period of optimization may unmask myocardial viability and refine revascularization strategies.
Functional mitral regurgitation as a marker of ventricular geometry
The parallel improvement in MR severity—from moderate-severe to mild-moderate—is consistent with reverse LV remodeling. Functional MR in ischemic cardiomyopathy is primarily driven by papillary muscle displacement, increased leaflet tethering and annular dilation (5). As LV geometry improves, tethering forces decrease, restoring leaflet coaptation. This case reinforces that functional MR is not a primary valvular disease but a ventricular disease, and its improvement can serve as a surrogate marker of reverse remodeling (6). An innovative takeaway here is the potential use of MR dynamics as a real-time, non-invasive indicator of myocardial recovery and treatment response.
Viability-guided CTO revascularization
Despite significant improvement, the persistence of symptoms and documented viability in the RCA territory justified reattempted revascularization. This aligns with contemporary evidence suggesting that: CTO PCI may improve symptoms, quality of life, and potentially LV function in viable territories [7). The benefit is most pronounced in patients with demonstrable ischemia or viability (8). In this patient, the presence of collaterals and regional hypokinesis (rather than akinesis) further supported myocardial viability.
This case supports a stepwise strategy:
1. Initiate GDMT and reassess ventricular function;
2. Evaluate myocardial viability;
3. Consider revascularization in symptomatic patients with viable myocardium;
Such an approach may optimize patient selection for PCI and procedural timing.
Timing of revascularization: Early vs deferred strategy
An important innovative perspective from this case is the concept of deferred CTO PCI after initial reverse remodeling (9). Immediate revascularization attempts may be technically challenging and less beneficial if myocardial stunning predominates. In contrast, delayed intervention: allows stabilization of the patient, improves procedural tolerance and may enhance myocardial recovery potential post-revascularization. This staged strategy is not yet standardized but may represent an important paradigm shift, particularly in young patients with newly diagnosed ischemic cardiomyopathy.
Young age and recovery potential
The patient’s young age (35 years) is a critical factor. Younger myocardium has greater plasticity and recovery potential, which likely contributed to the favorable remodeling observed. This highlights the importance of aggressive and persistent management in younger patients, even in the setting of severe initial dysfunction (10).
Conclusion
This case underscores the dynamic nature of ischemic cardiomyopathy and highlights several key clinical insights: Significant reverse LV remodeling and improvement in functional MR can occur with optimal medical therapy alone, even in the presence of a CTO. Functional MR should be viewed because of ventricular geometry, with its evolution reflecting underlying myocardial recovery. Viability assessment remains central in guiding CTO revascularization decisions. A deferred, stepwise approach to CTO PCI—after initial medical optimization—may enhance patient selection and outcomes. Young patients with ischemic cardiomyopathy represent a subgroup with high recovery potential and should be managed aggressively.
Overall, this case supports a personalized, physiology-driven strategy in CTO management, integrating myocardial viability, ventricular remodeling, and symptom burden to guide timing and necessity of revascularization.
Take home message
In young patients with ischemic cardiomyopathy and CTO, an individualized staged strategy combining aggressive GDMT, reassessment of ventricular remodeling, myocardial viability evaluation, and deferred CTO-PCI when symptoms persist may maximize myocardial recovery, improve functional mitral regurgitation, and optimize long-term clinical outcomes.
Ethics: Informed written consent was obtained from patients for all procedures and treatment. The case was managed in a compliance with Helsinki 2024 agreement on human studies.
Peer-review: External and internal
Conflict of interest: The authors declare that they have no competing interests.
Authorship: R.T., B.H. and K.K. equally contributed to case management, manuscript preparation and fulfilled all authorship criteria.
Acknowledgement and funding: None to declare.
Statement on A.I.-assisted technologies use: Authors used A.I. technology for preparation of graphical abstarct
Data and material availability: Does not apply
References
| 1.Reifart N. Challenges in complicated coronary chronic total occlusion recanalization. Interv Cardiol 2013; 8:107-11. doi:10.15420/icr.2013.8.2.107 https://doi.org/10.15420/icr.2013.8.2.107 PMid:29588761 PMCid:PMC5808620 |
||||
| 2.Leite L, Carlos T, Ferraz Costa G, Cruz I, Donato H, Silva R, et al. Effect of percutaneous coronary intervention on chronic total occlusions with documented viability or ischemia: A systematic review and meta-analysis. BMC Cardiovasc Disord 2025; 26: 17. doi:10.1186/s12872-025-05405-0 https://doi.org/10.1186/s12872-025-05405-0 PMid:41345829 PMCid:PMC12781582 |
||||
| 3. Huang AL, Dal-Bianco JP, Levine RA, Hung JW. Secondary mitral regurgitation: Cardiac remodeling, diagnosis, and management. Struct Heart 2022; 7: 100129. doi:10.1016/j.shj.2022.100129 https://doi.org/10.1016/j.shj.2022.100129 PMid:37273859 PMCid:PMC10236886 |
||||
| 4.Furquim SR, Sampaio de Sousa Lira MT, de Sá Pereira Belfort D, Biselli B, Chizzola PR, Munhoz RT, et al. Reverse Remodelling, Myocardial recovery and remission in heart failure with reduced ejection fraction: Clinical implications and management strategies. Card Fail Rev 2025; 11: e33. doi:10.15420/cfr.2025.41 https://doi.org/10.15420/cfr.2025.41 PMid:41523231 PMCid:PMC12784276 |
||||
| 5. Golba K, Mokrzycki M, Drozdz J, Cherniavsky A, Wrobel K, Roberts BJ, et al. Mechanisms of functional mitral regurgitation in ischemic cardiomyopathy determined by transesophageal echocardiography (from the Surgical Treatment for Ischemic Heart Failure Trial). Am J Cardiol 2013; 112: 1812-8. doi:10.1016/j.amjcard.2013.07.047 https://doi.org/10.1016/j.amjcard.2013.07.047 PMid:24035166 PMCid:PMC3830629 |
||||
| 6.Messas E, Bel A, Szymanski C, Cohen I, Touchot B, Handschumacher MD, et al. Relief of mitral leaflet tethering following chronic myocardial infarction by chordal cutting diminishes left ventricular remodeling. Circ Cardiovasc Imaging 2010; 3: 679-86. doi:10.1161/CIRCIMAGING.109.931840 https://doi.org/10.1161/CIRCIMAGING.109.931840 PMid:20826595 PMCid:PMC2987516 |
||||
| 7. Werner GS, Kim J-H, Hildick-Smith D, Kang D-Y, et al. Quality of life after percutaneous coronary intervention or medical therapy for chronic total coronary occlusions: EUROCTO and DECISION-CTO meta-analysis. JACC 2026; DOI: 10.1016/j.jacc.2026.02.5099 https://doi.org/10.1016/j.jacc.2026.02.5099 |
||||
| 8. Leite L, Campos G, Silva R, Jorge E, Oliveira-Santos M, Gomes A, et al. The association of collaterals with myocardial ischemia and viability in chronic total occlusions. Int J Cardiovasc Imaging 2023; 39: 843-51. doi:10.1007/s10554-022-02772-z https://doi.org/10.1007/s10554-022-02772-z PMid:36494504 |
||||
| 9. El Ghazawi A, Alwan M, Al-Mallah M. Selecting the right patient for CTO-PCI: is ischemia still the key?. Eur Heart J Imaging Methods Pract 2026;4: qyaf164. doi:10.1093/ehjimp/qyaf164 https://doi.org/10.1093/ehjimp/qyaf164 PMid:41523262 PMCid:PMC12781093 |
||||
| 10. Chrysakis N, Xanthopoulos A, Magouliotis D,Randall C. Starling, Drakos SG, Triposkiadis F, et al. Myocardial Recovery. Diagnostics (Basel) 2023; 13: 1504. doi:10.3390/diagnostics13081504 https://doi.org/10.3390/diagnostics13081504 PMid:37189604 PMCid:PMC10138096 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
