A rare case of cardiac tamponade by multiple pericardial hydatidosis
CASE REPORT
A rare case of cardiac tamponade by multiple pericardial hydatidosis
Article Summary
- DOI: 10.24969/hvt.2026.665
- CARDIOVASCULAR DISEASES
- Published: 08/07/2026
- Received: 31/03/2026
- Revised: 24/06/2026
- Accepted: 25/06/2026
- Views: 16
- Downloads: 4
- Keywords: Pericardiocentesis, pericardial hydatid cyst, pericarditis, anaphylaxis
Address for Correspondence: Amulya Cherukumudi, St. Johns Medical Hospital, Bangalore, India
Email: amulyac1@yahoo.com
Nihaz Nazir, Amulya Cherukumudi
St. Johns Medical Hospital, Bangalore, India
Abstract
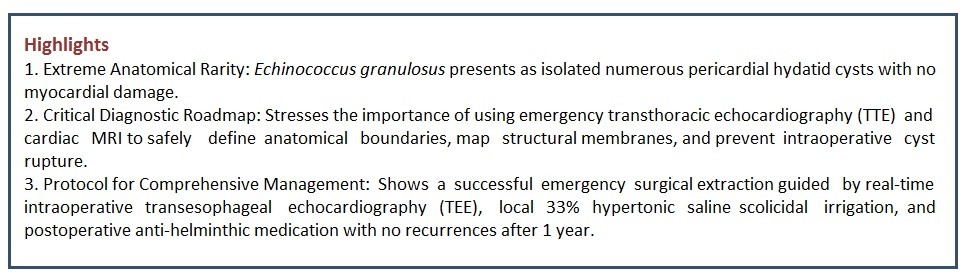
Objective: Cardiac hydatid cysts are relatively uncommon with incidence between 0.5-2% in patients with hydatid cysts. Most cardiac hydatid cysts are located either in the left ventricle or the interventricular septum. It can present in many ways, of which, multiple intrapericardial hydatid cysts resulting in pericarditis, pericardial effusion or even cardiac tamponade is rare. It is also noted that the disease along with its surgical management carries a high complication rate due to high risk of rupture causing anaphylaxis and death.
Case presentation: Here, we present the case of a 45-year-old man with multiple pericardial hydatid cysts leading to cardiac tamponade. An emergency transthoracic echocardiography was performed which revealed multiple loculated pericardial cysts with pericardial effusion compressing right side heart chambers. Surgery with removal of cysts and irrigation with hypertonic saline was done under transesophageal echocardiography guidance. The patient was prescribed and discharged on antihelmintic therapy.
Conclusion: Isolated multiple pericardial hydatid disease with presenting with cardiac tamponade is a rare entity. Early diagnosis and timely surgical management is the key for a successful outcome.
Key words: Pericardiocentesis, pericardial hydatid cyst, pericarditis, anaphylaxis
Introduction
Hydatid illness is a zoonotic parasitic infection induced by the larval form of Echinococcus granulosus. It persists as endemic throughout tropical and subtropical regions, encompassing the Middle East, India, Africa, South America, and Australia (1). Humans operate as unintentional intermediate hosts, contracting the infection by consuming food or water tainted with parasite eggs, or by direct contact with definitive canine hosts (1).
Upon ingestion, the oncospheres infiltrate the intestinal mucosa to access the portal or lymphatic circulation. The liver serves as the principal anatomical barrier, filtering around 75% of larvae, with the lungs accounting for 10% of cases (2). Cardiac involvement is infrequent (0.5–2%), predominantly affecting regions with substantial myocardial mass and vascular supply: the left ventricle (60%), interventricular septum, and right ventricle (3, 4). Isolated pericardial involvement that entirely spares the myocardium is an exceptional occurrence (3, 4). Despite their slow growth and prolonged clinical silence, these cysts provide a persistent risk of fatal consequences, including cyst rupture, severe anaphylaxis, and rapid cardiac tamponade (4).
Graphical abstract
Case report
A 45-year-old male patient presented to casualty with acute onset of breathlessness. Preceding this acute breathlessness episode, he gave history of cough with expectoration, dyspnea on exertion and easy fatigability for 3 months. On examination, patient appeared tachypneic with a heart rate of 104 beats/minute, blood pressure of 90/40 mm Hg, respiratory rate of 35 breaths/minute and saturation of oxygen as 95% on room air. He had pulsus paradoxus with raised jugular venous pressure, muffled heart sounds, bilateral crepitations present on auscultation of lung fields. This was associated with bilateral pedal edema and abdominal distension.
Patient provided written informed consent for all diagnostic and treatment procedure. The patient was and managed according to rules set by Helsinki 2024 agreement on human studies.
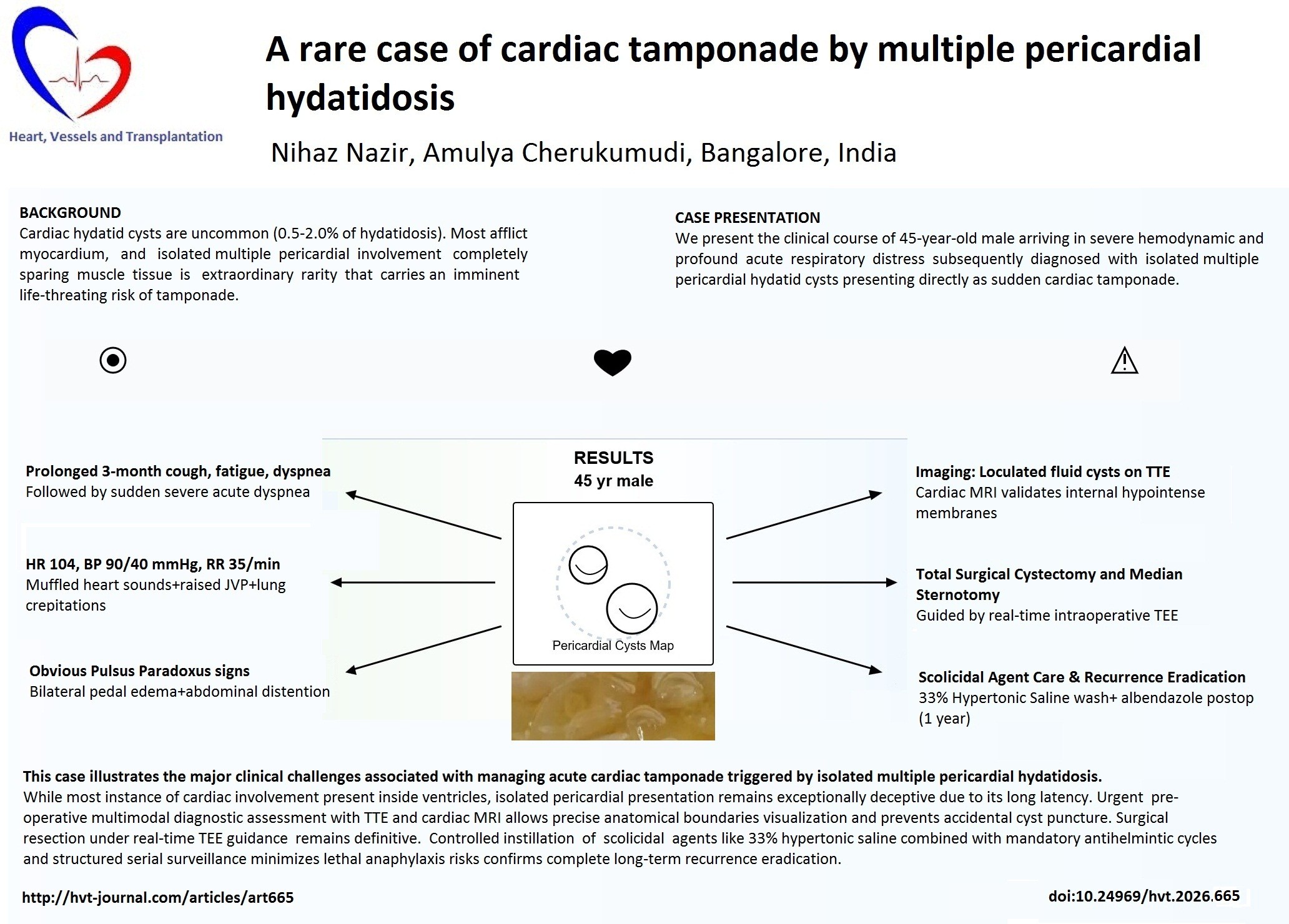
An emergency transthoracic echocardiography (TTE) was performed which revealed multiple loculated pericardial cysts with pericardial effusion compressing right-sided heart chambers (Fig. 1, 2).
Cardiac magnetic resonance imaging (MRI) showed multiple hyperintense areas of fluid collection with hypointense curvilinear membranes within it, causing cardiac tamponade.
The patient was started with dopamine 5 mcg/kg/min intravenous infusion for hypotension, injection of hydrocortisone 100 mg intravenously and chlorpheniramine 10 mg intravenously to prevent the anaphylaxis.
After a multidisciplinary meeting with cardiology, cardiothoracic surgery and infectious disease, the management was decided. First, with a large bore 16 G needle, thick yellowish fluid of about 250 ml aspirated. The pericardial cavity was then instilled with hypertonic saline (33%) to kill the scolices. The patient was observed further symptoms of tamponade or pulmonary edema and monitored closely for anaphylaxis. Patient was taken up for surgery under general anesthesia via a median sternotomy. Intra-operatively, massive pericardial effusion with thickened pericardium was noted, within which lay multiple cysts.
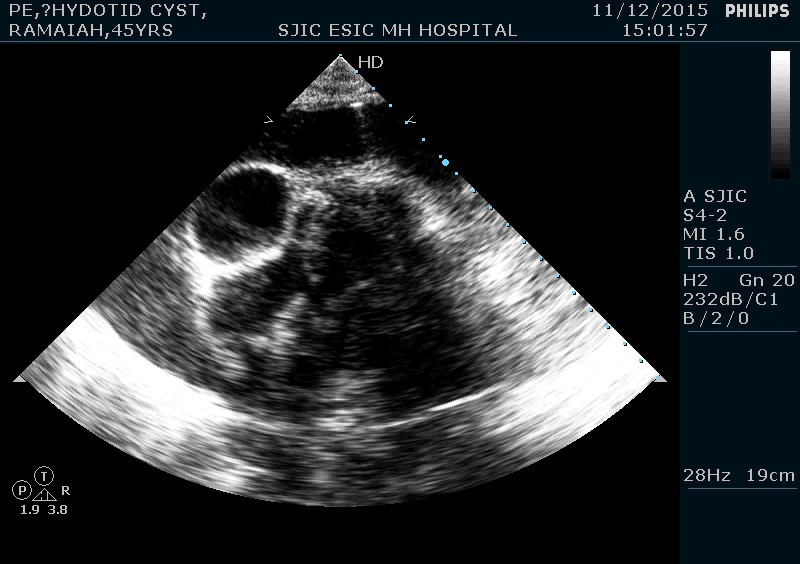
Figure 1. Two –dimensional echocardiography showing multiple fluid filled cystic lesions within the pericardium
Figure 2. Two –dimensional echocardiography showing the large cystic lesion measuring 3.68 x 4.45 cm compressing right atrium and ventricle
Transesophageal echocardiography (TEE) showed the same findings, guiding the surgeon adequately in cyst extraction without rupture.
The formal pericardiotomy was performed. Intraoperatively, the parietal and visceral pericardium was thickened, yet not altering hemodynamics. Several daughter cysts were noted within the pericardial cavity. These were removed in toto (Fig. 3)
Patient was shifted to cardiac intensive care unit with minimal inotropic support. The post-operative course was uneventful and patient was discharged from hospital on the 5th post-operative day. Patient is followed up regularly, with TEE after 1 year found to be devoid of any remnant cysts or recurrence.
Discussion
Isolated pericardial hydatidosis is a rare clinical phenomenon; most pericardial cysts documented in the literature arise from the rupture of a primary cardiac cyst (3-6). This case is notable due to comprehensive intraoperative and imaging assessments revealing isolated pericardial involvement while completely preserving the underlying myocardium.
Mechanisms of cardiac seeding
The larvae of Echinococcus granulosus traverse intricate circulatory routes to reach the heart.

Figure 3. Daughter cysts removed from the pericardial cavity
Although the majority of larvae are ensnared by the hepatic and pulmonary capillary networks, a subset evades these barriers to access the systemic circulation (1, 2). Larvae can enter the right heart either the inferior vena cava or the azygos vein (2).
To access the left heart and coronary circulation, they must traverse a patent foramen ovale or navigate the pulmonary capillary bed as micro-oncospheres (1-3).
In addition to systemic arterial administration through the coronary arteries, additional routes encompass direct lymphatic dissemination from neighboring mediastinal structures or direct hematogenous transfer via venous anastomosis (1, 2, 6). Upon entering the cardiopericardial region, the parasite encounters a richly vascularized milieu. Nonetheless, the reason it sporadically affects the pericardium while completely circumventing the high-flow left ventricular myocardium is an epidemiological enigma.
Comparative literature and complexities
In contrast to the traditional accounts by Blanton (2004) and Pedrosa et al. (2000), which characterize hydatid cysts as incidental parenchymal abnormalities in the liver or lungs, cardiopericardial hydatidosis manifests as a significant space-occupying lesion (1, 2). Although up to 90% of cardiac cysts may be asymptomatic due to their gradual growth, any mechanical disturbance poses significant dangers.
The case of our patient with acute cardiac tamponade exemplifies the most fatal expression of this condition. Historical cohorts indicate that problems such as spontaneous or trauma-induced cyst rupture pose a dual threat -
mechanical/hemodynamic: a rupture or swift fluid collection within the inflexible pericardial sac that induces quick tamponade (3, 4, 6, 7).
The abrupt discharge of highly antigenic hydatid fluid into the systemic or pericardial circulation incites extensive immunoglobulin (Ig) E - mediated degranulation, leading to severe allergy, unmanageable shock, and swift mortality (6, 8).
Diagnostic necessities and surgical strategy
Contemporary cardiac imaging has transformed the pre-operative management of this condition. Echocardiography, encompassing both TTE and intraoperative (TEE), is the primary diagnostic tool, proficiently detecting cyst movement, loculation, and direct chamber compression.
Cardiac MRI is essential for conclusive surgical planning. It offers enhanced tissue characterization, distinctly outlining the pathognomonic hypointense "double-line" sign of the pericyst, identifying daughter cysts, and accurately mapping the connection between the cyst wall and the coronary arteries (2, 6). This comprehensive anatomical guide mitigates the risk of inadvertent intraoperative rupture during sternotomy or tissue dissection (6).
Rationale for scolicidal agents
The intraoperative application of scolicidal drugs is a fundamental principle of hydatid surgery, ensuring optimal antiparasitic effectiveness while maintaining tissue safety. The release of living scolices into the pericardium during excision may result in significant secondary pericardial hydatidosis or lethal anaphylaxis (7, 8).
To mitigate this hazard, scolicidal agents such as hypertonic saline (15–33%) or ethanol (70–95%) are administered into the cystic cavity or utilized as irrigation agents (7, 8). Hypertonic saline functions by establishing a pronounced osmotic gradient that dehydrates and ruptures the invaginated scolices (7). It is essential to avoid extended systemic absorption or direct myocardial toxicity, hence localized, controlled instillation is the preferable method (7, 8).
Conclusion
Isolated multiple pericardial hydatid disease presenting with acute cardiac tamponade is an extremely rare, life-threatening clinical scenario. Rapid diagnosis utilizing emergency transthoracic echocardiography and cardiac MRI is paramount for anatomical delineation and meticulous surgical planning. Intraoperative transesophageal echocardiography serves as an invaluable tool to guide complete cyst extraction and avoid dangerous rupture.
Critically, a successful long-term outcome does not end in the operating room. To prevent aggressive local recurrence from occult micro-spillage, patients must receive postoperative anti-helminthic therapy (e.g., albendazole) paired with a structured, long-term follow-up regimen utilizing serial echocardiography (6).
Ethics: Patient provided written informed consent for all diagnostic and treatment procedure. The patient was and managed according to rules set by Helsinki 2024 agreement on human studies.
Peer-review: External and internal
Conflict of interest: None to declare
Authorship: N.N. and A.C. equally contributed to a patient management and preparation of case report, thus fulfilled all authorship criteria
Acknowledgements and Funding: None to declare
Statement on A.I.-assisted technologies use: Authors did not use A.I. in preparation of manuscript
Data and material availability: Not available
References
| 1, Blanton R. Echinococcosis. In: Behrman RE, Kliegman RM, Jenson HB, editors. Nelson Textbook of Pediatrics. 17th edition. Philadelphia: WB Saunders Company; 2004. pp. 1173-4. | ||||
| 2. Pedrosa I, Saiz A, Arrazola J, Ferreiros J, Pedrosa CS. Hydatid disease: Radiologic and pathologic features and complications. Radiographics 2000; 20: 795-817. https://doi.org/10.1148/radiographics.20.3.g00ma06795 PMid:10835129 PMCid:PMC11175755 |
||||
| 3. Perez-Gomez F, Duran H, Tamames S, Perrote JL, Blanes A. Cardiac echinococcosis: Clinical picture and complications. Br Heart J 1973; 35: 1326-31. https://doi.org/10.1136/hrt.35.12.1326 PMid:4759932 PMCid:PMC458802 |
||||
| 4. Kudaiberdiev T, Djoshibaev S, Yankovskaya L, Djumanazarov A. Multiple hydatid cysts of epicardium and pericardium. Int J Cardiol 2001; 81: 265-7. https://doi.org/10.1016/S0167-5273(01)00554-X PMid:11744146 |
||||
| 5. Noah MS, el Din Hawas N, Joharjy I, Abdel-Hafez M. Primary cardiac echinococcosis: Report of two cases with review of the literature. Ann Trop Med Parasitol 1988; 82: 67-73. https://doi.org/10.1080/00034983.1988.11812211 PMid:3041930 |
||||
| 6. Thameur H, Abdelmoula S, Chenik S, Bey M, Ziadi M, Mestiri T, et al. Cardiopericardial hydatid cysts. World J Surg 2001; 25: 58-67. doi: 10.1007/s002680020008 https://doi.org/10.1007/s002680020008 PMid:11213157 |
||||
| 7. Birincioğlu CL, Bardakci H, Küçüker SA, Ulus AT, Arda K, Yamak B, et al. A clinical dilemma: cardiac and pericardiac echinococcosis. Ann Thorac Surg 1999; 68: 1290-4. doi: 10.1016/s0003-4975(99)00692-x https://doi.org/10.1016/S0003-4975(99)00692-X PMid:10543495 |
||||
| 8. De Martini M, Nador F, Binda A, Arpesani A, Odero A, Lotto A. Myocardial hydatid cyst ruptured into the pericardium: Cross-sectional echocardiographic study and surgical treatment. Eur Heart J 1988; 9: 819-24. https://doi.org/10.1093/eurheartj/9.7.819 PMid:3169050 |
||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
