Method of septal myectomy in the surgical treatment of hypertrophic cardiomyopathy
MISCELLANEOUS
Method of septal myectomy in the surgical treatment of hypertrophic cardiomyopathy
Article Summary
- DOI: 10.24969/hvt.2026.644
- CARDIOVASCULAR DISEASES
- Published: 23/04/2026
- Received: 31/03/2026
- Accepted: 02/04/2026
- Views: 520
- Downloads: 391
- Keywords: Hypertrophic cardiomyopathy, method of myectomy, invention
Address for Correspondence: Kuat B. Abzaliyev, Al-Farabi Kazakh National University, Almaty, Kazakhstan
E-mail: kuatabzaliev1961@gmail.com
Innovations and patents
Method of septal myectomy in the surgical treatment of hypertrophic cardiomyopathy
Kuat B. Abzaliyev, Rustem M. Tuleutaev, Symbat A. Abzaliyeva, Roza T. Kuanyshbekova, Elena N. Pakhomenko, Almaty, Kazakhstan
Abstract
The invention relates to medicine, namely to cardiac surgery and can be used for surgical treatment of hypertrophic obstructive cardiomyopathy (HOCM).
The technical result of the invention is to provide it the following properties: efficient, fast, and safely performed septal myectomy, in which there is no development of complete block, formation of a defect in the septum and retention of residual stenosis.
The technical result of a method of septal myectomy in HOCM is based on excision through the aortic lumen hypertrophied myocardium of the left ventricular outflow tract, by inserting three needles in the projection of the part interventricular septum to be excised; through the lumen of the middle needle introduce ends of two 3/0 Prolene threads and exit through the lumens of the needles at the edge, where one more thread is inserted, the needles are removed, and the ends of the threads are taken on a tourniquet and pulled tightly, cutting through the thickness of the myocardium with the thread, which allows rapid, safe, reliable and effective septal myectomy without development of complete block and residual stenosis.
Key words: Hypertrophic cardiomyopathy, method of myectomy, invention
Graphical abstract
![]()

The invention relates to medicine, namely cardiothoracic surgery and can be used for surgical treatment of hypertrophic obstructive cardiomyopathy (HOCM). Various methods and modifications of septal myectomy are known (1-20).
Despite numerous modifications of this septal myectomy method, residual gradient or complete transverse block remains one of the formidable complications of the operation. The myectomy operation is dangerous because the septal wall is poorly visualized due to limited access through aortic root, which may lead to a high gradient persisting at the left ventricular outflow tract (LVOT), the formation of a defect in the septum with excessive resection and development of complete block. In addition, myectomy is associated with complications such as damage to the aortic and mitral valves, as well as incomplete relief of obstruction due to careless movement of the scalpel. Therefore, the surgeon faces the task of adequate, safe, and rapid resection of the hypertrophied myocardium.
The closest method is the method proposed by Akihiko Usui with coauthors in 2013 (11). He proposed a method of surgical treatment of HOCM, which consists in after opening the ascending aorta inserting three needles into the area of the hypertrophied tissue. One needle is inserted under the middle part of the right coronary leaflet. The second needle is inserted under the commissure between the right and left coronary leaflets of the aortic valve. The third needle is placed between the two previous ones. The needles are withdrawn into the left ventricular cavity, stepping back 2-3 mm from the fibrous ring of the aortic valve, and then the needles are stabilized with Kocher clamps. Resection of the hypertrophied tissue is performed in one block along the three needles from the aortic valve ring toward the apex of the left ventricle. Known septal myectomy methods have shown their effectiveness but require careful and gradual resection of the hypertrophied portion of the interventricular septum (IVST) using a scalpel, which can lead to the development of a complete transverse block, creation of a septal defect, or inadequate myocardial resection and development of residual gradient at the LVOT.
Known septal myectomy methods have shown their effectiveness but require delicate and gradual resection of the hypertrophied part of the IVST using a scalpel, which can lead to the development of a complete transverse block, creation of a defect in the septum or in contrast to insufficient myocardial resection and development of a residual gradient at the LVOT, which prolongs the operation and leaves the surgeon with doubts. The disadvantages of these septal myectomy methods are that:
1. The method does not guarantee the development of a complete transverse block or LVOT residual gradient.
2. The method leaves doubts and a sense of dissatisfaction in the surgeon.
3. To use known methods of surgery requires a long time to perform the myectomy, to avoid creating a defect in the IVST.
The objective of the invention is to develop a method of septal myectomy by inserting three needles into the area of the hypertrophied IVST in the projection of the presumed resection site and, through the lumen of the middle needle, feed ends of two 3/0 Prolene sutures and pull them out through the lumens of the needles at the edge where one more suture is fed; the needles are removed, and the ends of the sutures are taken on a tourniquet and firmly tightened, cutting through the thickness of the myocardium with the sutures, which allows for fast, safe, reliable, and effective septal myectomy without the development of complete block and residual stenosis.
The technical result of the invention is to confer the following properties: fast, safe, reliable, and effective septal myectomy, prevention of complete transverse block development, IVST defect, and residual stenosis.
The method was tested on 15 patients and showed 100% effectiveness, absence of all complications, whereas in the control group moderate residual stenosis (systolic gradient 8-10 mmHg) was observed in 1 patient (6.6%). The stated technical result is achieved by the fact that after the introduction of three needles into the projection of the resected part reliably and effectively perform septal myectomy without the development of complete block and residual stenosis. Thus, septal myectomy is performed efficiently, quickly, and safely, in which there is no development of complete blockade, formation of a defect in the septum, and leaving residual stenosis.
Method of septal myectomy in the surgical treatment of HOCM is depicted in Figures 1- 4.
Description of the method: After inserting three needles into the projection of the IVST part to be excised (Fig.1), into the lumen of the middle needle (Fig. 2) insert the ends of two 3/0 Prolene threads and bring them out through the lumen of the needles at the edge, where another thread is fed, the needles are removed, and the thread ends are taken on a tourniquet (Fig. 3) and pulled tightly, cutting through the myocardium thickness with the thread (Fig. 4).
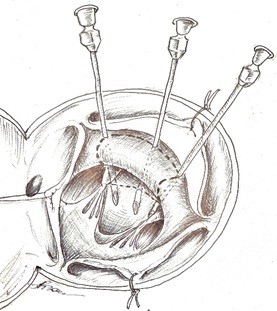
Figure 1. Insertion of three needles into the projection of the IVST part to be excised
IVST – interventricular septum
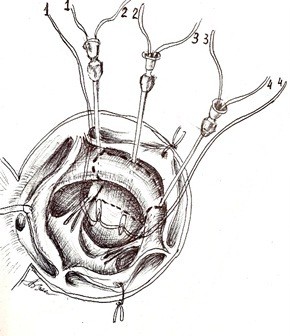
Figure 2. Insertion the ends of two 3/0 Prolene threads into the lumen of the middle needle and bringing them out through the lumen of the needles at the edge, where another thread is fed.
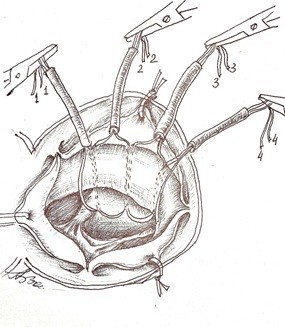
Figure 3. The needles are removed and the thread ends are taken on a tourniquet
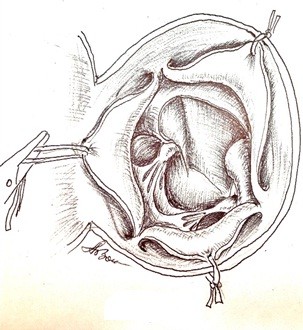
Figure 4. The threads pulled tightly cutting through the myocardium thickness
The use of the proposed method for hypertrophic septal myectomy in surgical treatment of HOCM will allow:
1. To avoid the development of complete transverse block, a defect in the IVST or residual gradient in the LVOT.
2. The method leaves no doubt or dissatisfaction for the surgeon.
3.The procedure does not require a prolonged time to perform the myectomy.
The proposed method permits effectively, quickly, and safely performing septal myectomy.
Formula of the invention
Method of septal myectomy in HOCM by excision through the lumen of the aorta of the hypertrophied myocardium of the LVOT, after inserting three needles in the projection of the IVST portion to be excised, is characterized by that through the lumen of the middle needle ends of two Prolene 3/0 threads are inserted and exit through the lumen of needles located at the edge, where one more thread is inserted, the needles are removed, and the thread ends are taken onto a tourniquet and pulled tightly, cutting through the myocardium thickness with the thread, which allows rapid, safe, reliable, and effective septal myectomy without development of complete block and residual stenosis.
As the authors we have obtained a certificate of entry into the state register of rights to objects protected by copyright for “Method for calculating the volume and area of septal myectomy in patients with hypertrophic cardiomyopathy and outflow tract obstruction of the left ventricle” No. 24261 dated 10.03.2022 (Fig. 5).

Figure 5. Authors certificate of invention No. 24261 issued on 10.03.2022
In the process of studying pathology on a computed tomography (CT), we obtain images (scans). Using the CT software, we can determine the radius of the hypertrophied part of the IVST (Fig. 6), and we can also draw and measure the line of the proposed excised part.
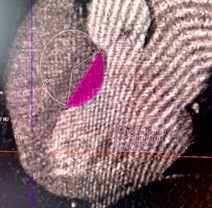
Figure 6. Computed tomography image: Determination of the radius of hypertrophied part for excision
The following Task 1 is set:
• find the area of the unsubtracted part (circle segment) shaded in pink at the condition that the radius (R) of the circle with center at point O and the length of the cut-off segment AB (Fig. 6) are known;
• find the volume of the cut-off body under the condition that the “thickness” of the cut-off segment is 2 cm.
Calculations for the resection of the left ventricular outflow tract part of IVST
For the above example, using the CT scanner software, we have:

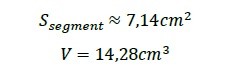
The area of the segment is defined by the formula:

General formula for finding the area using the given data:

Find the volume of the cut-off part by the formula:

where h is the thickness of the cut-off part.
General formula for finding the volume of the cut-off body:

Thus, by substituting the concrete values (1) and h=2 cm into formulas (2) and (3), we obtain the area and the volume of the cut-off body for Task 1:
In general, here we considered the simplest model of the shape of the cut-off body, namely the case when the cut-off part is a cylinder segment with the base area found above and height (thickness) h – given.

Let us consider a less simplified model.
Imagine a CT scan as a sheet of paper with the following picture:

We need to find the area of the excised part in this plane of section – the shaded circular segment. From the scan data, we know the lengths of segments [OA], [OB], [AB]. Above we gave formula (1) for finding the area of such a segment.
Next, the CT can perform such scans with a step of 1 mm, i.e. we will have 20 scans, describing the shape of the pathology (assuming its “thickness” is 2 cm). We then use the analogy of a scan with a sheet of paper (or thick cardboard – each sheet thickness 1 mm) with an image. If we stack all scans, we will obtain a stack of sheets in which the shaded areas form a part of the heart septum that must be excised. The task is to find the volume of this region. In our model considered, above, the excised part represents a segment of a cylinder, i.e., did not change along the entire the radius (thickness) of the excised body.
Assume that in the cross-sections of the body there are also circular varies, i.e. a certain function. Suppose we obtained the following image (if viewed in the “profile” of the excised part):
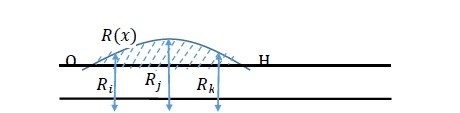
where Ri, Rj, Rk - radii of the corresponding sections, and Rx– a function describing the change of the radius.
The volume of the resulting shaded figure representing the excised body can be found in two ways:
a) Note that the resulting figure is a surface of revolution of the Rx function around the OH axis. In this case the volume of the excised part can be found by the
b)
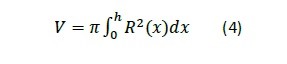
Suppose, for example, that the OH curve is a parabola described by the equation

Then from formula (4) and with h=2 we have:

c) We have 20 scans corresponding to the excised area. Take the first scan - according to the algorithm described above, we find the area of the first segment, multiply it by the scan step (say, 1 mm), obtaining some volume V1 and, the same is done with the second scan – we will obtain V2, etc.
Next, we will sum up to obtain the volume of the entire part to be excised:
Thus, we built mathematical models described by formulas (4) and (5) for calculating the area and volume of the excised part in pathology for the case when the excised body is a shape of rotation.
The indicated models can be used in further research on constructing mathematical models for septal myectomy in patients with hypertrophic cardiomyopathy and outflow tract obstruction and other pathologies in surgery, when using and constructing computer 3D models in medicine. The examples discussed can also be used to create computer programs to assist surgeons in calculating parameters of the excised part – area, volume, mass. The authors also filed and applied for an invention patent and received patent No. 36227 dated 26.05.2023.
Peer-review: Internal
Conflict of interest: None to declare
Authorship: K.B.A., R.M.T., S. A. A., R.T.K., and E. N.P equally contributed to the preparation of manuscript and thus fulfilled authorship criteria
Acknowledgements and Funding: None to declare.
Statement on A.I.-assisted technologies use: Author stated they did not use artificial intelligence (A.I.) tools for writing manuscript
Data and material availability: Does not apply
References
| 1.Ommen SR, Mital S, Burke MA, Day SM, Deswal A, Elliott P, et al. 2020 AHA/ACC Guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2020; 76: e159-240. doi: 10.1016/j.jacc.2020.08.045 https://doi.org/10.1016/j.jacc.2020.08.045 PMid:33229116 |
||||
| 2.Ommen SR, Ho CY, Asif IM, Balaji S, Burke MA, Day SM, et al. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR Guideline for the management of hypertrophic cardiomyopathy: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2024; 83: 2324-405. doi: 10.1016/j.jacc.2024.02.014. https://doi.org/10.1016/j.jacc.2024.02.014 PMid:38727647 |
||||
| 3.Monda E, Rubino M, Lioncino M, Di Fraia F, Pacileo R, Verrillo F, et al. Hypertrophic Cardiomyopathy in Children: Pathophysiology, Diagnosis, and Treatment of Non-sarcomeric Causes. Front Pediatr 2021; 9: 632293. doi: 10.3389/FPED.2021.632293 https://doi.org/10.3389/fped.2021.632293 PMid:33718303 PMCid:PMC7947260 |
||||
| 4.Timmis A, Gale CP, Flather M, Maniadakis N, Vardas P. Cardiovascular disease statistics from the European atlas: inequalities between high- and middle-income member countries of the ESC. Eur Hear Journal Qual Care Clin Outcomes 2018; 4: 1-3. doi: 10.1093/EHJQCCO/QCX045. https://doi.org/10.1093/ehjqcco/qcx045 PMid:29177406 |
||||
| 5.Wang Z, Zheng Y, Ruan H, Li L, Zhang M, Duan L, He S. The impact of hypertension on the prognosis of patients with hypertrophic cardiomyopathy: a single-center retrospective study. Peer J 2023; 11: e14614. doi: 10.7717/PEERJ.14614 https://doi.org/10.7717/peerj.14614 PMid:36650838 PMCid:PMC9840863 |
||||
| 6.Gudkova AYa, Rybakova MG, Bokeriya LA, Shlaychto EV. Hypertrophic cardiomyopathy. Clinico-morphological comparisons. Arch Pathol 2012; 74: 8-11. | ||||
| 7.Arbelo E, Protonotarios A, Gimeno JR, Arbustini E, Arbelo E, Barriales-Villa R, et al. 2023 ESC Guidelines for the management of cardiomyopathies: Developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC). Eur Heart J 2023; 44: 3503-626. Doi: 10.1093/EURHEARTJ/EHAD194 https://doi.org/10.1093/eurheartj/ehad194 PMid:37622657 PMCid:PMC13040680 |
||||
| 8.Frustaci A, Russo MA, Chimenti C. Diagnostic contribution of left ventricular endomyocardial biopsy in patients with clinical phenotype of hypertrophic cardiomyopathy. Hum Pathol 2013; 44: 133-41. doi: 10.1016/j.humpath.2012.04.023 https://doi.org/10.1016/j.humpath.2012.04.023 PMid:22939960 |
||||
| 9.Geske JB, Sorajja P, Ommen SR, Nishimura RA. Variability of left ventricular outflow tract gradient during cardiac catheterization in patients with hypertrophic cardiomyopathy. JACC Cardiovasc Interv 2011; 4: 704-9. doi: 10.1016/j.jcin.2011.02.014 https://doi.org/10.1016/j.jcin.2011.02.014 PMid:21700258 |
||||
| 10.Yan LR, Zhao SH, Wang HY, Duan FJ, Wang ZM, Yang YJ, et al. Clinical characteristics and prognosis of 60 patients with midventricular obstructive hypertrophic cardiomyopathy. J Cardiovasc Med 2015; 16: 751-60. doi: 10.2459/JCM.0000000000000163 https://doi.org/10.2459/JCM.0000000000000163 PMid:25022933 |
||||
| 11. Usui A, Araki Y, Oshima H, Ueda Y. А needle stick technique for septal myectomy for hypertrophic obstructive cardiomyopathy. Ann Thorac Surg 2013 Feb; 95: 726-8. https://doi.org/10.1016/j.athoracsur.2012.09.085 PMid:23336896 |
||||
| 12.Ferrazzi P, Spirito P, Iacovoni A, Calabrese A, Migliorati K, Simon C, et al. Transaortic chordal cutting: Mitral valve repair for obstructive hypertrophic cardiomyopathy with mild septal hypertrophy. J Am Coll Cardiol 2015; 66: 1687-96. doi:10.1016/j.jacc.2015.07.069 https://doi.org/10.1016/j.jacc.2015.07.069 PMid:26449139 |
||||
| 13.Morrow AG, Brockenbrough EC. Surgical treatment of idiopathic hypertrophic subaortic stenosis: technic and hemodynamic re- sults of subaortic ventriculomyotomy. Ann Surg 1961; 154:181-9. https://doi.org/10.1097/00000658-196108000-00003 PMid:13772904 PMCid:PMC1465878 |
||||
| 14.Elliott P M, Anastasakis A, Borger M A, Borggrefe M, Cecchi F, Charron P, et al. 2014. ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy. Russ J Cardiol 2014; 5:7-57. doi: 10.15829/1560-4071-2015-5-7-57 https://doi.org/10.15829/1560-4071-2015-5-7-57 |
||||
| 15.Gusak AA. Reference manual for problem solving: Mathematical analysis and differential equations. Minsk: TetraSystems 2003. | ||||
| 16.Hattori M, Aoki T, Sekioka K. Differences in direction-dependent shortening of the left ventricular wall in hypertrophic cardiomyopathy and in systemic hypertension. Am J Cardiol 1992; 70: 1326-32. https://doi.org/10.1016/0002-9149(92)90770-Y PMid:1442586 |
||||
| 17.Maron B. Relation between extent of cardiac muscle cell disorganization and left ventricular wall thickness in hypertrophic cardiomyopathy. Hypertrophic cardiomyopathy systematic review. JAMA 2002; 287: 1308-320. https://doi.org/10.1001/jama.287.10.1308 |
||||
| 18.Sagintaev SS, Sagintaeva SS. Higher mathematics. Almaty: Almaty University of Power Engineering and Telecommunications 2020. | ||||
| 19. Spiridonov SV. Surgical treatment of obstructive forms of hypertrophic cardiomyopathy. Available at: URL: http://cardiolog.org/ | ||||
| 20. Babokin VE, Martakov MA, Zainetdinov EM, Popov MA. Method of surgical treatment of hypertrophic obstructive cardiomyopathy. Patent 2017 RU 2 621 167 C1. | ||||
Copyright

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
AUTHOR'S CORNER
